


Sarah Atkins1, *, Sally Fowler Davis2
1Clinical Specialist Occupational Therapist (Dip COT SROT) Sheffield Teaching Hospitals NHS Foundation Trust
2Associate Professor Organization in Health and Care, Sheffield Hallam University and Sheffield Teaching Hospitals NHS Foundation Trust
*Corresponding Author: Sally Fowler Davis, Associate Professor Organization in Health and Care, Sheffield Hallam University
Abstract
People with tetraplegia are rightly expecting that digital technologies will allow them to compensate for an element of their personal impairment. Technologies can enable people to navigate environmental challenges, access on-line products and provide information about services. Occupational therapists (OT’s) working with people who have spinal injuries need to be aware of digital devices and methods that can support their patients and facilitate the process of deploying technology, enabling the adoption by people in varying stages of their adaptation to disability. A rapid literature review was undertaken within an NIHR clinical academic internship: To gain a critical understanding of technology adoption in the practice of OT with people who have post-acute spinal injury. The study demonstrated a limited focus on the personalized deployment of 'smart' technologies. The Technology Adoption Model (TAM) was used to synthesize findings, based on the key principles that acceptance of technology is based on devices or methods that are a) unobtrusive, b) high performance, c) required little or no maintenance and d) where a device achieved practical restorative functional gains. Studies showed that setting up technologies for example, environmental control systems was a lengthy process that required a technical skill that was highly varied in the patient population. People disabled with spinal injuries who chose to adopt technology reported strong benefits associated with successful use yet had to overcome difficulties with learning, maintenance, and lack of technical support.
Keywords: environmental controls, spinal cord injury, digital technology, adoption of computer
Introduction
Digital Technologies Including
The personal computer, mobile telephones, tablets, and the internet are now embedded in the day-to-day living in the UK and other Organisation for Economic Co-operation and Development (OECD) countries. There is a recognition that the value to individuals is matched by economic benefits in terms of gross domestic product for connected countries [1]. Digital methods provide new methods of communication, control of everyday devices and play an increasingly essential role in work and leisure. They benefit the user by enabling them to undertake a range of daily activities, including study, and employment, and wider communication wherever there is a sufficient internet connection. The demand for 'smart' home-based digital technologies to enable activities of daily living is also being articulated by people with tetraplegia. Navigating a home; opening curtains, doors, regulating heating, and home devices are now within smart home technologies [2]. Vocational rehabilitation often depends on computing capabilities [3] with self-management invariably depending on social media, networking sites, and home-based internet [2]. OTs working within Spinal Injury Centres and N.H.S assistive technology teams, together with those working within charities such as Aspire, seek to provide rehabilitation to people who have been paralyzed by Spinal Cord Injury, helping them move from injury to independence. Aspire, who fund technology, volunteers, and assistive technologists to work within Spinal Cord Injury Centres, have debated the usefulness of mainstream smart home technologies for people with spinal cord injuries [4]. The technology debate includes concerns regarding compatibility, maintenance, and reliability of devices, particularly where the supply of equipment is dependent on internet connectivity. Risks are understood to be based on poor universal coverage, unreliable wi-fi and practitioner can be apprehensive about devices that fail, particularly in an emergency. At this time, the NHS environmental control provision criteria include traditional environmental control systems but do not include mainstream smart home technology [5]. This highlights the need for OTs to incorporate an understanding of digital technology adoption into their practice, to be able to advise on products and services, as part of treatment planning. This is based on a professional commitment to enable patients to engage in the occupations they value and overcome the barriers presented when they cannot access technology [6]. Use of assistive technology has long been used as a tool by occupational therapists to enable a return to daily occupations [7].
Assistive technology is defined as “any piece of equipment, or product, whether it is acquired commercially, modified or customized; that is used to increase maintain or improve the functional capabilities of individuals with disabilities”[8]. In 2013 The World Health Organisation (WHO) and International Spinal Cord Society Report [9], highlighted the value of allocating resources to enable people with Spinal Cord Injuries to access assistive technology. They advise that assistive technology is beneficial to maximize independence, including using Environmental Control Systems. These enable control over the immediate environment such as the T.V. computer, telephone lights, and doors. They advocate the use of computer technology to provide access to information on the internet, a method of communication, participation in education, work, and leisure. Also, they emphasize that assistive technology provides economic benefits to society by reducing the costs associated with care and unemployment. In addition to traditional assistive technologies specifically designed for people with disabilities, global advances in technology have resulted in, commercially available methods of controlling the environment and accessing a computer, which does not require hand function and can be retrofitted to the home environment to enable independence and quality of life [2]. The mainstreaming of home-based digital controls depends on the assessment of the benefits of the on-line service or device, i.e., enhancing daily living providing additional control or functionality beyond the norm, or the additional vulnerability i.e., remotely monitoring utilities or reducing security risks. In some cases, the assessment includes personal preferences for social connectivity via remote communication methods and on-line networks. A major factor in the assessment is an individual's willingness to accept technology as part of their normal routine. The Technology Acceptance Model (TAM) is one of the few methods proposed as a useful predictor of technology acceptance. This behavioural model was developed in the 1980s to understand information technology use in the workplace. It states that the information technology user’s acceptance is influenced by; their pre- use beliefs regarding perceived usefulness and ease of use, which leads to their attitude, intention to use, and actual use [10].
Digital Assistance Within Spinal Cord Injury
A previous systematic review reported on the use of computers and task performance at home for people without upper limb movement associated with tetraplegia [11]. They found that assistive technology devices such as voice command software, modified mice, switches, and typing sticks could be used to provide access to computers and controlling the home environment. The review concluded that people with spinal cord injury who used assistive technology for computer access believed that they had a better quality of life with improved participation, independence, and self-esteem. Some people with spinal cord injuries are interested in commercially available mainstream technology are becoming interested in the application of further digital services and devices; also expressing a level of frustration with traditional assistive technologies available through NHS provision,[12,13]. This stimulus contributed to the completion of this study, undertaken within a National Institute of Health Research (NIHR) Pre-Masters Clinical Academic Internship Programme [5].
The Review Question: What is influencing the acceptance and adoption of computer / digital technology and environmental controls within the community-dwelling spinal cord injured tetraplegic population?
Methodology
A rapid review methodology was selected and completed in six months of clinical academic development. Rapid reviews are an assessment of what is already known by using systematic review methods. This is accomplished by setting out a protocol to focus the question and set out the scope and limits of the search. The rapid review is rigorous and explicit and thus systematic but makes concessions to the breadth or depth of the process by limiting particular aspects of the systematic review process [14]. The study was devised using the PICOS tool. This was the most appropriate tool for a fully comprehensive search where time and resources are limited [15].
The PICOS Tool Was Used as Follows
The search aimed to identify literature about people with tetraplegia, due to spinal cord injuries, using assistive technology; computers, and or environmental controls in the community who have used technology or rejected the use of technology. To capture the most recent evidence about advances in technology only literature from the last 6 years was included.
P = Population; tetraplegia, quadriplegia, and spinal cord injuries
I = Intervention; assistive technology, computer, digital technology, smart technology, self -help device, the internet, environmental controls
C= Context; community-dwelling
O= Outcome; technology adoption, technology non-adoption, technology acceptance, technology non-acceptance.
S= Study type; all types of studies, published in peer-reviewed sources including reported user experience within studies.
The search terms were, “tetraplegia”, “quadriplegia”, “spinal cord injury”, “spinal cord injuries” and assistive technology. The connector “NOT” was used to exclude types of assistive technology specific to walking, mobility, standing, pressure ulcers, infertility, driving, showering, bathing, hygiene, and other conditions resulting in paralysis cerebral palsy, and stroke. Searches conducted to test additional terms; computer, smart technology, self-help device, internet, environmental controls did not produce additional references. To meet the criteria of “community-dwelling” the study participants needed to be no-longer in hospital. Studies conducted in a laboratory experimental environment were also excluded because this study seeks to explore what is accessible and practical for the individual living with spinal cord injury at home. A range of literature reporting on early-stage experimentation and design of new methods for controlling computers such as brain control interfaces, tongue operated assistive systems, vision-based interfaces, and body machine interfaces using inputs from jaw movements, shoulder motion, and facial position and expression were also excluded. These were not selected for review because the research did not relate to the community setting; views of people living with spinal cord injuries (adoption of technology) and the technologies when not available outside of the laboratory setting. The exception to this was a large- scale survey that sought to assess the pre-use attitudes of the tetraplegic spinal cord injured population to technology that was included. Studies based on community-dwelling participants were easily separated from those based in hospitals. Studies excluded were also those not relating directly to adult spinal cord injury or tetraplegia, those technologies not directly enabling access to environmental controls and or computers, and those not published in English. Electronic searches used the following databases Scopus, IEEE, CINHAL complete, MEDLINE, PsycINFO, Google Scholar. Besides, an individual search of the British Journal of Occupational Therapy was carried out and some literature was sourced by word of mouth from health professional colleagues. The references of relevant articles found were searched for further relevant articles. A PROSPERO search was carried out on 02.12.18 and no registered relevant prospective studies were found. The study was not registered because as a rapid review it is accepted as a preliminary investigation. Ethics approval is not required for a literature review [16]. A Critical Appraisal Skills Programme Checklist was used with each article to ensure appropriateness and rigor for inclusion [17]. Articles were included where they provided valuable comments from users on the use and non -use of technology or on pre-use attitudes for community- dwelling participants. A data extraction sheet formulated by the first author used the headings; Population, Intervention, Context, Outcome, Study Type, Themes Identified by authors, funding, additional thoughts. Additional headings derived from the Technology Acceptance Model (TAM), discussed as useful were used for analysis. These were TAM perceived usefulness, TAM perceived use, TAM attitude, TAM intention to use/ acceptance, and actual use. The data extraction sheet and key findings were reviewed by the second author.
Results/Findings
Literature was selected if it met all the inclusion criteria and none of the exclusion criteria as summarised in the PRISMA flow diagram (Figure 1). 218 records were identified after duplicates were removed. After screening by title and abstract 85 articles were screened for eligibility. Full-text versions were obtained of all relevant articles and evaluated for inclusion according to the criteria. These were collated by the first author in a spreadsheet tabulating the relevance to the search protocol, this was reviewed by the second author. Six studies were agreed as suitable for inclusion. Data extraction was undertaken to identify the salient elements of the literature about the TAM- From the data extraction sheet, (Table 1 and Table 2) and subsequently, the key findings were identified. Due to small-scale studies with a qualitative design and only one large- scale survey, the level of evidence was not suitable for a meta- analysis. The five qualitative studies using interview methods had low numbers of participants; Folan et al. [3] had 3 community-dwelling participants, Hooper et al. had 5 participants [2], Myburg et al. had 15 participants [18]. In the first study by Verdonck, M. et al (2014) [19] there were six participants and then further analysis of five of those participants was reported in a further study published in 2018. Therefore, the total number of participants from these studies was 29. Of these only five were women, although this is not unexpected within a spinal cord demographic. A higher proportion of men is thought to be representative of the UK Spinal Cord Injured Population [19]. The studies were carried out in Australia [3,2,18] and The Republic of Ireland [20,21]. They all had convenience or purposive samples. The numbers were not large enough to analyse according to each level of injury. The sixth study was a large survey, studying 156 participants with tetraplegia due to traumatic spinal cord injury [3]. This sought to assess the pre-use attitudes of the spinal cord injured population in the United States of America, using a range of theoretically presented Brain Control Interfaces. The participants were 18- 81 years old. They had received C1- C7 injuries 40 % of which were complete. This data was subdivided into groups C1-4 with 54 participants, and C5 – C7 with 102 participants. All were stated to be due to traumatic causes with time since injury ranging from one month to 62 years. The proportion of males to females was not stated. The participants were recruited from the community, via advertisements using websites, paper adverts, and using forums, and support groups for people with spinal cord injuries. The large numbers of participants and recruitment from several sources add weight to the relevance of the findings for the American population. But the data were presented as percentages without any statistical analysis to aid consideration of the level of bias.
The survey [3] sought to ascertain user attitudes towards eight technologies. There were 13 theoretical control opportunities including three relating to accuracy and speed of typing and two relating to control and accuracy of a computer cursor. The survey sought to assess the attitudes of the participants towards using technology to achieve benefits gave the burdens of each system, using a 5-point Likert scale, to rate the likelihood of use. The results of the survey [3] showed that respondents were concerned about the appearance of devices, issues with daily maintenance, and the potential requirement for technician intervention. For brain control interfaces to achieve widespread adoption they need to allow unobtrusive, high performance, autonomous use and require little or no maintenance. When rating the potential output control opportunities there was a preference for achieving restorative functional movements. However, a substantial 80 % of C1- C4 people with tetraplegia injured for 10 years or more were likely to adopt technology if it could naturally control a computer cursor. This figure was 56 % for those injured for 10 years or more in the C5-7 group. The study did not document the user's reasoning behind this difference between the higher-level and lower-level groups. A possible further study is needed to investigate the hypothesis that the C5-7 group, who have more upper limb function, can use other devices already. Further framework analysis using the Technology Acceptance Model and themes identified by the authors [22], results are presented in (Table 2). In TAM perceived usefulness and perceived ease of use, feed into the users' attitudes towards technology. Within the literature analyzed participants saw technology as useful for completing tasks independently [23] with specific goals including controlling a mainstream mobile telephone or tablet [12], autonomous control of the home environment [18], and natural control of a computer cursor [3]. Participants pre-use ease of use expectations were that; for technology to be accepted, they wanted it to be fast, accurate, and natural [21]. Technologies that do not require maintenance or carer intervention and be unobtrusive are preferred [21]; however, the evidence was that in reality setting up environmental controls systems was lengthy, with technical issues and required reprogramming and that troubleshooting was required by someone with hand function and additional training was insufficient [18]. Assistive technology to access computers was found to be challenging and slow to use with participants' pre-injury level of knowledge of computers being variable. The users with less knowledge found learning harder [3]. In line with TAM theory, participants attitude to technology showed a clear interplay of usefulness and ease of use [2] describes “opportunities and costs” [18] described that the device, “has to pass a threshold of practicality over options such as asking a carer for help” [24] also described this as; “The interplay between hassle and engagement”.
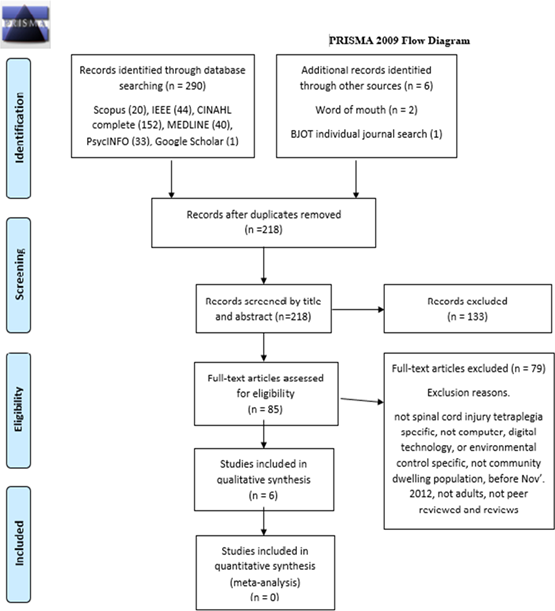
Figure 1: PRISMA 2009 Flow Diagram
Table-1
|
Reference |
Population |
Intervention |
Context |
Outcome |
Study Type |
|
Folan A, Barclay L, Cooper C, Robinson M. Exploring the experience of clients with tetraplegia utilizing assistive technology for computer access, Disability Rehabilitation, Assistive Technology 2015 Jan 2 10(1): 46-52. |
Participant numbers =7. Traumatic Spinal cord injury. (C4-C5 Tetraplegia ASIA A or B) Adult males 20-60 years. 6-48 months post-injury. Range of level of education from left school Y9 - tertiary degree. 4 inpatients. 3 community-dwelling. |
Assistive technology for computers uses Dragon voice activation, trackball mouse, finger splints, quad joy, mouse grid. |
Victorian Spinal Cord Service, Royal Talbot Rehabilitation Centre, Melbourne Australia.
All participants studied were assistive technology users, non-users were not studied. |
Participants.
had an increased sense of control over their lives… enhanced self-efficacy and quality of life. Further research should include a study into non- use. |
Qualitative. Purposive sampling. 30 min semi-structured interviews (face to face or by telephone, transcribed, analyzed for themes (inductive process). Transcript and theme checking with the participants. |
|
Hooper B, Verdonck M, Amsters D, Myburg M, Allan E. Smart-device environmental control systems: experiences of people with cervical spinal cord injuries. Disability and Rehabilitation: Assistive Technology. 2018 Nov 17;13(8):724-30. |
Participant numbers =5. All had a Spinal Cord Injury. Level of injury; Tetraplegia C3 AIS B, 2x C4 AIS B, C4 AIS C, C5 AIS A, Adult Males 21yrs - 60, 3 in their early 40's |
Housemate smart device environmental controls. Access via tablet or smartphone with direct touch (the two C4 AIS B) or Sip/puff or combined sip puff with chin control. |
Existing user’s experiences with smart device environmental control systems. Queensland, Australia, use at home. Purposive sample from a state-wide rehabilitation service. This study only looks at existing users, not non-adoption. |
Participants report the ability to access mainstream smart device functions, increasing their, independence, choice, control, and connection to family and the outside world. Costs include money, time, and technical limitations causing frustration. Prescribers should find ways to mitigate these costs. Users report a reduction in carer burden because they could call for help. |
Qualitative, purposive sampling.semi-structured interviews in participants' own homes. Inductive thematic analysis. Reflexive journals and field notes. Single embedded case study method.Phenomenology. |
|
Myburg M, Allan E, Nalder E, Schuurs S, Amsters D. Environmental control systems–the experiences of people with spinal cord injury and the implications for prescribers. Disability and Rehabilitation: Assistive Technology. 2017 Feb 17;12(2):128- 36. |
Participant numbers =15. 12 male,3 female. Spinal cord injury tetraplegia. Level of injury; C2-C5 AIS A-D. 22-68 years. Educational level not stated. Personal lifestyle (carer) support hours 33- 168hrs/ week. Only 2 living alone. |
Progress TM, and Control 4. Device access method via; Direct access, sip and puff, chin control, specs switch, jellybean button, mouth-stick, microlight. All users had fully funded ECS via a government or insurance. Prescription by occupational therapy at the Queensland Spinal Cord Injuries Service. |
People were discharged from the Princess Alexandra Hospital Spinal Injuries Unit, in Brisbane Australia. All community-dwelling participants had been prescribed an environmental control system. |
- The importance of client readiness for the prescription. client perceptions of value, convenience and aesthetics influenced use. Prescribers should. -seek to understand what each client needs to become engaged, be proficient with use and knowledgeable about devices, prepare clients for difficulties, provide support until use is established. Provide follow-up and evaluation. |
Qualitative inquiry. 15 semi-structured interviews. Conducted in the home environment or over the telephone. Descriptive phenomenology. Purposive sampling. Coded transcripts. Field diaries. Data management software was used. |
|
Verdonck M, Steggles E, Nolan M, Chard G. Experiences of using an Environmental Control System (ECS) for persons with high cervical spinal cord injury: the interplay between hassle and engagement. Disability and Rehabilitation: Assistive Technology. 2014 Jan 1;9(1):70-8. |
6 participants with C3- C6 Spinal Cord Injury Tetraplegia. Level of injury completeness not stated. Inclusion criteria- inability to use a standard remote control and inability to feed themselves. 5 traumatic injuries and one spinal arteriovenous malformation. 3-35 years post-discharge. No current access to an environmental control system. Intelligible speech. 2 female,4 male. 22yrs-65yrs of age. |
Environmental control system (ECS) starter pack. A dynamic display infrared ECS controller (KEO), ability switches, mounts, telephones, an infrared electrical socket, sound operated personal alarm. Supporting video and instruction booklet. Control of– televisions, DVDs telephones, lamps, and fans. Customized to their preferences. 8week trial period. A stand-alone system not linked with smart devices. |
Participants; All community-dwelling 2 rural, 4 urbans. One living in a nursing home. 5 lived at home with family. All selected from a database held by Spinal Injuries Ireland. |
ECS use was engaging enjoyable and fun. Successful engagement involves overcoming hassle. Some hassle resulted in non- use. But non-use is not a failure, if based on experience and informed choice. Equipment trials are needed in early rehabilitation to establish habitual use. The experience of carers and family members warrants further study. ECS assessment and provision should be seen as an essential part of rehabilitation. |
Qualitative. Trial of a starter pack for 8weeks. Semi-structured interviews analyzed using Interpretive Phenomenological Analysis. Heuristic framework by Smith et al. Computer-assisted data analysis (CAQDAS). Thematic identification using I Mind Map. |
|
Verdonck M, Nolan M, Chard G. Taking back a little of what you have lost: the meaning of using an Environmental Control System (ECS) for people with high cervical spinal cord injury. Disability and Rehabilitation: Assistive Technology. 2018 Nov 17;13(8):785-90. |
Further analysis /discussion of the study above [Verdonck M et al. 2014] but only investigating the 5 participants who chose to use the technology, not the one participant who did not. |
As above. |
Participants were. All community-dwelling, One living in a nursing home. 4 were living at home with family members. All selected from a database held by Spinal Injuries Ireland. |
ECS use enables people to do everyday things, supports them to feel less dependent. facilitates a sense of security, promotes positive self-perception and continuity of being. Reclaiming a little doing promotes subjectively significant improvements in identity, relationships, and well-being. "Feeling enabled" was enjoyable and empowering leading to an increased sense of safety and reduced neediness.
|
Qualitative. Trial of starter pack - 8weeks. 5 participants semi-structured interviews analyzed using Interpretive Phenomenological Analysis. Heuristic framework by Smith et al. Computer-assisted data analysis (CAQDAS). Thematic identification I Mind Map. Further analysis of the 5 participants who chose to use ECS in the original study [Verdonck, M et al 2014]. Fieldnotes. Reflexive journals. |
|
Blabe CH, Gilja V, Chestek CA, Shenoy KV, Anderson KD, Henderson JM. Assessment of brain-machine interfaces from the perspective of people with paralysis. Journal of neural engineering. 2015Jul 14;12(4):043002. |
The number of participants=156. Spinal cord injured tetraplegics. Ages, 18-81 years. Time post-injury 1 month - 62 years. Levels of injury ranged from C1 - C7. 40 % complete injuries. All injuries were due to trauma. Results were grouped according to the level of injury; C1-4 (54 participants) and C5-C7 (102 participants). |
Survey of user preferences for 8 Brain-machine interface technologies including electroencephalography (EEG), Electrocorticography (ECoG), and intracortical microelectrode arrays, compared with an eye-tracking system. Presented to the participants as written theory and diagrams.13 hypothetical opportunities to provide function including typing, controlling a computer cursor, a robot, a robotic arm, a wheelchair, or their arm. |
Community-dwelling spinal cord injured participants. Recruited via advertisements on websites and in paper adverts using SCI forums and support groups. |
For devices to be widely adopted they need to be autonomous, unobtrusive, require little or no maintenance, and offer high performance. Most respondents wanted to restore natural movement. 80 % of C1 - C4 participants injured for 10 years or more and 56% of all C5-7 participants 10years plus post-injury; were likely to adopt a technology if it could naturally control a computer cursor. |
A survey using a 5-point Likert scale to rate the likelihood of use. |
Table 2: Data Extraction TAM and themes
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
TAM Actual use |
Themes and conclusions identified by the authors. |
|
Folan A, Barclay L, Cooper C, Robinson M. Exploring the experience of clients with tetraplegia utilizing assistive technology for computer access. Disability and Rehabilitation: Assistive Technology. 2015 Jan 2;10(1):46-52. |
Completing tasks independently.
Returning to life roles.
Experiencing normality.
Distraction from injury. |
Learning to use was slow, challenging, and frustrating.
The time needed to practice skills before technology became useful enough to participate in occupations.
Level of previous use - some not competent using computers preinjury. |
Participant's interest in technology was dependent on their psychological state. Participants referenced having processed suffering and starting to move towards a reformulated future. |
Returning to life roles and participation in meaningful occupations was a powerful motivator.
Making sense of their altered condition. “I use them because I have to, not because I want to.” |
Difficulties were overcome computer use became enjoyable.
Users reported a sense of control and empowerment. Ability to complete tasks independently.
Actual use: Facebook, school- work, skype, email, YouTube, online banking, work tasks, ordering supplies searching for products. Research medical and health information.
Self-management-organizing their daily schedule.
Return to work - one participant placed a high value on the use of the computer AT because it enabled employment - making big money. |
Getting back into life Completion of tasks independently. Return to meaningful life roles. Improved opportunities, to return to work. Assisting in adjusting to the injury. Overcoming physical barriers caused by the injury. Making sense of the altered condition caused by spinal cord injury. The technology was a distraction from injury enabling an ability to look forwards to the future.
Learning new skills. Can take a long time. Early introduction in rehabilitation is required. Is not limited by familiarity with computers.
Conclusions People with tetraplegia can be assisted to return to previous life roles or engage in new roles, through developing skills in the use of assistive technology for computer access. This ability led to an enhanced sense of self-efficacy and quality of life. |
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
Actual use |
Themes and conclusions identified by the authors. |
|
Hooper B, Verdonck M, Amsters D, Myburg M, Allan E. Smart-device environmental control systems: experiences of people with cervical spinal cord injuries. Disability and Rehabilitation: Assistive Technology. 2018 Nov 17; 13(8): 724-30.
|
Participants cited their desire to control a mainstream mobile phone or tablet as the main reason for obtaining a smart device ECS. |
Hard to determine from the evidence presented. All participants were selected because they had accepted Smart ECS use. |
Hard to determine from the evidence presented. All participants were selected because they had accepted Smart ECS use. |
Difficulties regarding financial cost. Learning to use was time-consuming. Slow speed scanning through options or changing mode for different options. Installation frustration. Lack of support and information from prescribers. Technical limitations - battery maintenance, poor blue tooth connectivity, short infrared range. Compatibility issues with other smart devices and appliances. Inability to use existing apple phones/ tablets resulting in had to purchase an android device. Having to learn to use android devices (phone) when they previously apple devices. |
The stated use. Independent choice and control over aspects of their environment. Decreased reliance on others and increasing time spent alone. Peace of mind for the user and carer due to the ability to call for help. Ability to utilize the resources of their paid carers' time more effectively. The Smart device replaced multiple devices being used separately to achieve the same functions. The advantages over a traditional Environmental control system were, the ability to use a mobile device to phone, message, use apps including playing games, social media, internet. Enabling more meaningful connections with the outside world (family abroad). |
Themes - Opportunities and Costs. Opportunities were.
Independent control, Choice, Peace of mind, connection, effective resource use, control over phone and apps.
Costs were.
Money, time investment, and dealing with technical limitations and resulting frustration.
Conclusions
Smart device environmental control systems offered a new opportunity for users to access mainstream smart device applications and functions. These facilitate connection to family and the outside world.
Prescribers and installers must consider ways to mitigate the costs experienced by users.
Future research should investigate methods and resources that practitioners could utilize to better support new users of smart device ECS. |
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
Actual use |
Themes and conclusions identified by the authors |
|
Myburg M, Allan E, Nalder E, Schuurs S, Amsters D. Environmental control systems–the experiences of people with spinal cord injury and the implications for prescribers. Disability and Rehabilitation: Assistive Technology. 2017 Feb 17;12(2):128-36.
|
Autonomy controlling the home environment. For participants to see their device as useful, it had to pass a perceived threshold of practicality over other options such as asking a carer for help. |
The process of setting up the ECS was lengthy - took months. Technical issues and reprogramming - only 4 participants described the process as smooth/straightforward. For troubleshooting -you need someone with a hand function.
User training was reliant on the knowledge of the O.T. there were no online forums or technical support.
|
Divided opinion on readiness /timing of prescription.
Users who were prescribed an environmental control system well before discharge were unable to make decisions about what they wanted before discharge - not ready to absorb information, overwhelmed, not sure what they wanted out of anything. Where the process of prescription was imposed on them this caused frustration disengagement and for some resigned acceptance.
Others regretted a late start wanting the ECS set up and functioning for discharge to enable independence and safety. |
Independence has positive psychological effects. Less asking alleviates the sense of being a pain to others. Decreased frustration of asking others improved wellbeing. When the system was not working it created feelings of uselessness and frustration. The environmental control system (ECS) was a critical enabler of spending time alone, especially at night. The goal to complete household tasks was not met by traditional ECS for this a mainstream device was needed to enable access to internet email and computer functions. Utilization was strongly influenced by the amount of hassle involved in positioning and moving the device. Many participants asked others to use the device, especially the switch scanning users because it is slow. The dated and obtrusive appearance of devices reinforced feeling disabled. |
Items controlled by the systems; Bed, air conditioning, lamp, wired light, fan ceiling & pedestal, phone landline, TV, DVD, stereo, auto door, personal alarm. But most devices had no access to computers/ internet tablets (they were traditional Environmental control systems) only one person was able to access a mobile phone via their device. Useful for controlling entertainment devices - especially allowing them to change their mind (music, TV). Some found ways to accomplish tasks in an easier, way than using their system e.g., touch lamps. When it was set up to control a safety device there was no contention as to its utility. Helped alleviate discomfort, pain, and boredom (entertainment, and bed controls). Unreliability is cited as a reason for abandonment in some cases. |
Readiness to engage with Environmental control systems Divided opinion on the correct timing of prescription. Perceptions of autonomy Independence has positive psychological effects. Training Training is critical to the successful adoption of the ECS. Training is required for occupational therapists, users, carers family, and friends. The utility of the environmental control system The system needs to work simply and efficiently or it's more trouble than it is worth. Vulnerability - problems lead to a sudden loss of independence. When it worked well it reduced stress and frustration for users and carers. Mainstream technology looks better than disability technology and this reinforces feeling disabled. Implications for prescribers. Prescribers should be knowledgeable, seek to understand what each client needs, prepare clients for potential difficulties in establishing reliable use and establish ongoing support mechanisms. |
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
Actual use |
Themes and conclusions identified by the authors |
|
Verdonck M, Steggles E, Nolan M, Chard G. Experiences of using an Environmental Control System (ECS) for persons with high cervical spinal cord injury: the interplay between hassle and engagement. Disability and Rehabilitation: Assistive Technology. 2014 Jan 1;9(1):70-8.
|
The user's expectations of the system pre-trial were not explored. Participants were contacted and asked to try. However, there was some evidence of usefulness exceeding their expectations. Participants reported not expecting the technology to be useful or personally relevant. ECS use was not routinely trialed In Ireland before discharge from rehabilitation. All participants had become accustomed to dependency. |
User's expectations of ease of use were not gathered pre- trial. But there is evidence of it being easier to use than expected. |
Dependency was tolerated and disliked. They experienced difficulty (described as hassle), changing dependency habits. Participants described frustration with the technology itself, technical issues, learning how to use it, and taking too long. Frustration with scanning as an access method. Frustration with supply issues through the healthcare system. Attitude to the technology changed positively for those participants that found it enabled them to do more. Participants reported that it just looked like part of their wheelchair, not the expected eyesore. Users compared the trial pack with older static display types and stated it was easier and nice. |
Agreement to participate in the trial created an intention to use for the study. For the study environmental controls (ECS) were only loaned for a trial period. Participants were supported with applications post-trial. But when assessed under the healthcare system, participants were frustrated about negotiations regarding the ECS being included as part of their care packages and delays. One participant received her prescribed ECS during the study. She had not seen it or trialed its pre-installation but reported she was not disappointed, she just wished she had had it sooner (36 years post-injury). The delay had been so long she had forgotten she had applied for one.
|
Users described play-fullness for example, turning the lamp on just because. Enjoying the surprise of others when they answer an incoming phone call. Users found autonomy with the controlling environment led to altered roles. James's parents were surprised by his ability to be alone. 5 out of 6 participants stated the autonomy was worth the hassle. The 6th Patrick had limited goals of access to tv channels and volume. His wife was always close and quicker (injured 19 years). Users described the ECS as a drug that gives pleasure and fosters dependency. They feared living without it at the end of the trial. Therefore, there is a transfer of dependency on a carer to a machine. This study describes non -use in the form of Patrick as well as use. |
Two major interlinked themes; "Getting used to ECS" which when achieved led to “Taking back a little of what you have lost”. Getting used to ECS had two sub-themes entitled hassle and engagement. Hassle had two elements changing habits and frustration. The engagement had 3 elements good feeling, fun and humor, and surprise. Conclusions People with high cervical spinal cord injuries find the environmental control system used to be engaging enjoyable and fun. Successful engagement with environmental control systems involves overcoming “hassle”. For some, environmental control systems may be too much hassle resulting in non- use. However, it is important that non-use is not necessarily considered a failure, provided it is based on real experience and well-informed choice. Realistic trials need to be made available early in rehabilitation to establish environmental control use and avoid habitual dependency on carers. |
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
Actual use |
Themes and conclusions identified by the authors |
|
Verdonck M, Nolan M, Chard G. Taking back a little of what you have lost: the meaning of using an Environmental Control System (ECS) for people with high cervical spinal cord injury. Disability and Rehabilitation: Assistive Technology. 2018 Nov 17;13(8):785-90.
|
As above same study. |
As above same study. |
As above same study. |
As above same study. The participants were all accustomed to physical dependence on others and technology alone was not seen as a safe substitute. However, participants reported feeling "Less needy". They reported feeling less frustrated, less annoyed, less of a burden. Consequently, less indebted to others and less obliged to show constant gratitude. Previously Bridget would choose to do without to avoid putting the carer under pressure. |
Increased ability to make preferred, spontaneous choices. Being alone provided space, "Just to have my own space because I never have my own space" (Matthew). ECS enabled participants to relish privacy once more. Frustration was described when the ECS needed maintenance. ECS enabled participants to enjoy their own space because they felt safe. But all still needed a carer close by they could call with the ECS or by voice. It helped participants feel more relaxed and reduced feelings of vulnerability by providing an ability to call for help quickly. |
Theme 1 "Reclaiming a little doing" - this reflected pleasure in being able to do everyday things again, enjoying one’s own company, and being less dependent. Theme 2 "Feeling Enabled" Encompassed experiencing pleasure in doing, feeling safe alone, and feeling less needy. Also feeling good and feeling better about oneself. ECS enabled participants to enjoy their own space because they felt safe. Conclusions While ECS use produces only a little objective change in activity levels, it subjectively means a lot to people with high-level injuries. ECS enables people to do every -day things as well as supporting them to feel less dependent and needy. Using ECS facilitates a sense of security. It helps promote positive self-perception and continuity of being. Those with high cervical spinal cord injury need to have access to ECS so they can enjoy the psychological and physical benefits. |
|
Reference |
TAM Perceived Usefulness |
TAM Perceived ease of use |
TAM Attitude |
TAM Behavioural intention to use Acceptance |
Actual use |
Themes and conclusions identified by the authors |
|
Blabe CH, Gilja V, Chestek CA, Shenoy KV, Anderson KD, Henderson JM. Assessment of brain–machine interfaces from the perspective of people with paralysis. Journal of neural engineering. 2015 Jul 14;12(4):043002.
|
A substantial number of participants were interested in brain-machine interfaces to provide access to technology, although they rated a return of normal upper limb movement as the highest functional outcome desired. The group of participants injured more than 10 years expressed the most interest in using Brain-Machine Interfaces to control a computer cursor. - for respondents with levels C1-4 80% were interested -respondents with levels C5-7 56% were interested. |
Perception of ease of use was important this included a requirement for lack of maintenance, unobtrusiveness, and lack of carer intervention. Participants responded that for technologies to be adopted they need to be fast accurate and natural.
|
This population was interested in Brain-Machine Interfaces as a method of improving function. The appearance of the device had a large influence on the likelihood of technology adoption with 90% likely to adopt eye-tracking glasses rather than wearing a wired device to the head, a cap, or having a brain implant. Surgically implanted wired devices were twice as likely to be adopted than their wired externally worn equivalents. |
This cannot be ascertained from the study, because the technology was only presented to the participants in theory. The cost implications for each device were not discussed. |
Actual use was not investigated in this study. Because the technology was not available for the participants to use. |
Understanding the needs of the spinal cord injured population is of paramount importance in the design of brain-machine devices.
Respondents were concerned about appearance, daily maintenance, and the potential need for technical intervention.
For brain control systems to achieve widespread adoption they need to be autonomous, unobtrusive, and require little or no maintenance. They must provide high performance.
In terms of output, there is a preference for restoring natural movement. There was a substantial number interested in controlling a computer. There was an enthusiasm in the spinal cord injured population for further development of brain-machine interfaces. |
Participants Reported the Following Themes about Usefulness and Challenges to Ease of Use
Usefulness
- The technology-enabled users achieve independence with everyday activities [3,2,18,24,21].
- A sense of safety by being able to call for help with environmental controls [2,18,24,21] and the resultant psychological benefit from being able to spend time alone [2,21].
- Computer access enabled a return to previous life roles as well as new ones including work [3].
- Modern “Smart” environmental control use enables telephone, messaging, social media, and computer access allowing valued access to the outside world [2].
- Users preferred mainstream devices because they look less disabled [18].
- Assistive technology use was enjoyable [3,24,21] and helped alleviate discomfort, pain, and boredom [18].
- Environmental control users felt less of a burden to their carers [18,21].
Challenges to Ease of Use
- Assistive technology users found learning time-consuming and frustrating [3,2,24,21].
- Frustration with technical issues and maintenance [2,18,24,21].
- Lack of technical support [2,18]
- Poor prescriber knowledge [2]
- Due to a psychological response to injury and trauma, the introduction of technology as an inpatient was too soon for some participants [3,18].
- Where technology was introduced long after hospital discharge participants were used to dependency and the changing habit was a hassle [24].
- Difficulty with ease of use. Switch scanning is slow [18].
- Dated and obtrusive the appearance of devices reinforced feeling disabled [18].
TAM outlines that attitude becomes 'intention to use’ and 'actual use' [10]. In all of the studies where participants used the technology participants chose to accept and use the devices trialed, with the exception of one participant in Verdonck et al. 2014 [18]. He is described as having expressed only one goal of being able to change television channels. It is reported that his wife was always nearer and quicker! But also, he had the technology introduced 19 years post-injury by which time he had developed dependency which was perhaps difficult to change.
Discussion
This study sought to identify the international literature related to technology adoption in people with a severe and enduring disability who may want and need to regain an element of control of their environment following impairment. The complex nature of technology adoption across different healthcare systems is an important topic for OTs working with clients who are accommodating to disability [25]. This includes the assessment of the acceptability of digital services and devices and the range of purpose and uses for people with spinal injury, across the world. It is also important to recognize that whilst some devices are tested in a research context, the application is dependent on access via purchase or procurement on the open market or through health provision. This study focuses on the latter, the adoption of technology outside the research environment. People with spinal injuries who chose to adopt technology reported strong benefits associated with successful use yet had to overcome difficulties with learning, maintenance, and lack of technical support [3,2,18,24,21]. The focus of OT has generally been to assess individuals' functional needs and to match the technology to their requirements; what works well for them to achieve particular functional goals. This depends on the level of injury and the opportunities and limitations within the community/ home environment. An additional requirement with the emergence of mainstream digital services is to make the patient aware of the enabling methods and services that could supplement their care, providing that they are willing to accept technology-based solutions. This variation in the willingness and ability to use technology is an additional part of the assessment process as OTs co-design the home with the patient and enable the patient and their family to prioritize resources and become an expert in selecting the most appropriate technologies.
This research draws in the experiences of successful assistive technology users, providing further information about the range of ways that a patient responds to digital devices in the community. The barriers to using or non-adoption are also highlighted but this evidence is limited by the fact that the majority of the studies [3,2,18,24,21] used purposive sampling and therefore may have reduced the number of patients who were non-adopters. The literature reviewed demonstrates that participants displayed a strong interest in technology to achieve autonomous computer access and control the environment. Including the view that mainstream technology was more desirable because its appearance was not additionally stigmatizing and normalized the user in society. This evidence is somewhat limited by small numbers of participants and purposive sampling [3,2,18,24,21]. Whilst impossible to generalize this result is important and reflects the potential of technology to enable full participation in community and a further degree of independence and self-management; profoundly changing the expectations of disabled living [26]. The survey [9], had large numbers of participants but gauged their pre-use beliefs and needs only and did not include any statistical analysis. In 2018 a Parliamentary committee reviewed the use of mainstream technology versus traditional assistive technology to enable people with disabilities to return to work [27]. They found that assistive technology was a critical employment resource with benefits for the user and economy. They found that traditional assistive technology was outdated and recognized the value of mainstream technology. This adds weight to the need to investigate which mainstream technologies work well for which groups of users. The matching Person with Technology (MPT) model [28] is an alternative model that could be used to assess the needs of the user and apply these to technology selection. Significantly the MPT includes a perspective on the timing of the adoption which is not included in the Technology Acceptance Model [10]. For disabled people returning to employment, the TAM is useful because it relates specifically to computer technology that can be applied to all populations and applied within a rehabilitation context.
Study participants placed value on their devices not only to achieve the expected independence goals but also to report psychological benefits from being able to be alone [2,21]. The qualitative studies showed a depth of evidence in some narrative accounts of people using devices including “freedom because if you can’t get out of bed you can still talk to people’ (Tom) and “It has allowed me to work and allowed me to make money, and good money” (Jarred) [3]. Similarly, important, being alone is enabled by using a digital device to call for help if needed and highlights the importance of the ways that mainstream technologies need to be consistent and reliable, even in the context of potentially unreliable internet connections. The Technology Acceptance Model [10] applied to the literature was found to be useful for highlighting how users’ attitude to technology influences the likelihood of successful continued use of the equipment. The Needs Assessment Checklist is a recognized assessment tool and outcome measure for people with Spinal Cord Injuries [29]. This is used to structure rehabilitation to focus the team on providing a patient-centered goal-setting approach which is essential to facilitate good outcomes. The psychological response to injury and trauma often means that the introduction of assistive technology during inpatient assessment is too soon for some future users [3,18]. Furthermore, inpatient participants were not yet sure about perceived use due to injury-causing an altered state of being [3]. Yet for others, the introduction seemed to be too late with participants who had been at home for 3 – 35 years being used to dependency on carers. [24]. Further research is needed about the transference of dependency from carer to technology, as it becomes accessible talking about [29], Reports of participants benefitting from not being dependent on their careers, such as feeling less of a burden [18,21] and the benefit of being alone [2, 21] are significant here.
The timing of an assistive technology intervention has been usefully critiqued [22] who addressed the importance of adoption within a wider outcome’s framework. This work recognized the importance of managing the expectations of the user in the delivery of assessment services and also the capability of the user in the planning for technology. It is highly relevant to this review that the conceptual framework for technology preparation and adoption is used in occupational therapy practice to improve person-centered outcomes [28]. The pervasiveness, complexity, and sophistication of technology are increasing at a phenomenal rate and while this growth is enabling technology to play a more prominent role in supporting people living with life-limiting conditions and their care partners in a wide variety of ways, it is more critical than ever to consider who chooses and advises on the adoption [29]. One of the models discussed in Gitlin’s model (1998): Biopsychological framework and concept of career, as a person with disability [30]. It identifies a pathway of changing needs as the user progresses from novice as an inpatient through early user at home to experienced user and expert user. It highlights the different needs of the user at different stages and importantly the concept of a change in “environmental fit” at home. This concept of suitability for use in the environment is a common theme throughout all the six models discussed by Lenker et al. [30]. The conclusion of this review was, “The lack of a fully realized predictive model for assistive technology outcomes research indicates the need for development and validation” [31]. A more recent review [17] reported that new conceptual models of assistive technology are under development and Scherer’s Matching Person with the technology model (MPT) was the most mentioned. This has three guiding elements. Technology – its functions and characteristics, Social medium/environment, personal and psychosocial factors. The International Spinal Cord Society states that “without outcomes research in the area of assistive technology for people with spinal cord injury, it will be difficult to determine what works, how well it works and for whom it will work” [8]. Since there was no evidence found relating to the U.K. population there is a need for further research. There is a standard for classifying the neurological level and extent of spinal cord injury, The American Spinal Injury Association Impairment Scale (AIS A-E), (International Perspectives on Spinal Cord Injury page 30), this will enable future researchers to compare which technologies work best for each level of injury.
Strengths and Limitations
- The studies which explored actual technology use [3,2,18,24,21] had low numbers of participants, so it is not possible to draw conclusions about which technologies work well for each level of injury or any demographic group.
- Within the published literature there were no studies relating to participants within the United Kingdom.
- This study aimed to take a contemporary view and so the literature reviewed was limited to within the last 6 years. This may have excluded some literature relevant to the discussion relating to technology acceptance and adoption.
- Some critical factors have been explored that serve to promote the assessment, acceptance, and adoption of computer / digital technology and environmental controls.
- The study limited scope to those in the community seeking to use technologies and has not explored hospital-based technology use.
Conclusions
People with Spinal Cord Injuries are beginning to provide compelling testimonies of the benefits of assistive technology to access computers and control their environments. The literature associated with the adoption of digital assistive technology in the community is somewhat limited but practical aspects associated with individual need and capability are clear. New users need support, over a period of time, to enable them to benefit from the range of devices available. The role of the OT is to assess the user’s capability and capacity by exploring their priorities for occupations and activities and to be sufficiently knowledgeable about the usefulness of the technology in the context/home environment. This study was an initial inquiry into evidence that could support OT practices and services within a UK Spinal Injury Unit and potentially inform how service users might engage with and adopt technology in their rehabilitation. The goal was to highlight the process of technology adoption when the person with Spinal Cord Injury is psychologically receptive and in the right supportive environment for them. There is a need to increase access to digital technologies to enable patients to express opinions and priorities for ways to overcome new impairments. Technology adoption has not so far been explored fully by Occupational Therapists and this study is important because it highlights the need for a radical approach to the knowledge, understanding, and capability of practitioners to advocate for people living with disabilities; to independently participate in a society where digital technology is increasingly becoming part of daily living. Technology has the potential to promote increased self-esteem and economic benefits such as employment. Further research is needed to investigate which technologies work well for people, according to the level of injury within the community environment. The review identifies a gap in studies that inform digital technology adoption by people with spinal cord injury and the best practice by rehabilitation practitioners in the U.K
Conflict of interest: No other conflict of interest.
Key Findings
Technology adoption is an important factor in the assessment of the usefulness and benefits derived from digital devices and methods. People with Spinal Cord Injury experience barriers to using digital devices and further research is required to investigate which technologies work well for people, according to the level of injury, within the community environment.
What the Study Has Added
The review identifies a gap in studies that inform digital technology adoption by people with Spinal Cord Injury and the best practice by rehabilitation practitioners in the U.K.
References
- Welfens PJ, Perret JK (2014) Information & communication technology and true real GDP: economic analysis and findings for selected countries. International Economics and Economic Policy 11(1-2): 5-27.
- Hooper B, Verdonck M, Amsters D, Myburg M, Allan E (2018) Smart-device environmental control systems: experiences of people with cervical spinal cord injuries. Disabil Rehabil Assist Technol. 13(8): 724-730.
- Folan A, Barclay L, Cooper C, Robinson M. Exploring the experience of clients with tetraplegia utilizing assistive technology for computer access. Disabil Rehabil: Assist Technol, 10(1): 46-52.Aspire Spinal Injuries Charity (2019).
- Aspire Spinal Injuries Charity (2019).
- NHS England Service specifications Spinal Cord Injury (2019).
- Liu L (2018) Occupational therapy in the Fourth Industrial Revolution. Canadian Journal of Occupational Therapy 85(4): 272-283.
- Polgar JM (2006) Assistive technology as an enabler to occupation: What's old is new again. Canadian Journal of Occupational Therapy 73(4): 199-204.
- International Spinal Cord Society. International perspectives on spinal cord injury (2013).
- World Health Organization and International Spinal Cord Society (2013). International perspectives on spinal cord injury.
- Holden RJ, Karsh BT (2010) The technology acceptance model: its past and its future in health care. J Biomed Inform 43(1): 159-172.
- Baldassin, V, Shimizu HE, Fachin-Martins E (2018) Computer assistive technology and associations with quality of life for individuals with spinal cord injury: a systematic review. Qual Life Res 27(3): 597-607.
- Prospero National Injuries Unit, Osborn Building, Northern General Hospital, Herries Road, Sheffield. S5 7AU – Inpatient feedback.
- NHS England Service specifications complex disability environmental controls (2018).
- Grant MJ, Booth A (2009) A typology of reviews: an analysis of 14 review types and associated methodologies. Health Information & Libraries Journal, 26(2): 91-108.
- Methley AM, Campbell S, Chew-Graham C, McNally R, Cheraghi-Sohi S (2014) PICO, PICOS and SPIDER: a comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC health Serv Res. 14(1): 579.
- Prospero National Institute for Health Research.
- Critical Appraisal Skills Programme (CASP) part of Oxford Centre for Triple Value Healthcare (2019).
- Myburg M, Allan E, Nalder E, Schuurs S, Amsters D (2017 ) Environmental control systems–the experiences of people with spinal cord injury and the implications for prescribers. Disability and Rehabilitation: Assist Technol. 12(2): 128-136.
- Verdonck M, Steggles E, Nolan M, Chard G (2014) Experiences of using an Environmental Control System (ECS) for persons with high cervical spinal cord injury: the interplay between hassle and engagement. Disabil Rehabil Assist Technol 9(1): 70-78.
- Savic G, DeVivo MJ, Frankel HL, Jamous MA, Soni BM, et al. (2017) Long-term survival after traumatic spinal cord injury: a 70-year British study. Spinal Cord 55(7): 651-658.
- Blabe CH, Gilja V, Chestek CA, Shenoy KV, Anderson KD, et al. (2015) Assessment of brain–machine interfaces from the perspective of people with paralysis. J Neural Eng 12(4).
- Fuhrer MJ, Jutai JW, Scherer MJ, DeRuyter F (2003) A framework for the conceptual modelling of assistive technology device outcomes. Disabil Rehabil 25(22): 1243-1251.
- Verdonck M, Nolan M, Chard G (2018) Taking back a little of what you have lost: the meaning of using an Environmental Control System (ECS) for people with high cervical spinal cord injury. Disabil Rehabil Assist Technol 13(8): 785-790.
- Verdonck MC, Ryan S (2008) ‘Mainstream Technology as an Occupational Therapy Tool Technophobe or Technogeek?’, British Journal of Occupational Therapy 71(6): 253–256.
- Lewin D, Adshead S, Glennon B, Williamson B, Moore T, et al. (2010) Assisted living technologies for older and disabled people in 2030. A final report to Ofcom. London: Plum Consulting.
- Department of Work and Pensions Committee, House of Commons (2018).
- Lenker JA, Paquet VL (2003) A review of conceptual models for assistive technology outcomes research and practice. Assist Technol. 15(1): 1-15.
- Kennedy P, Smithson E, Blakey L (2012) Planning and structuring spinal cord injury rehabilitation: the needs assessment checklist. Top spinal cord inj rehabil, 18(2): 135-137.
- Lenker JA, Fuhrer MJ, Jutai JW, Demers L, Scherer MJ, et al. (2010) Treatment theory, intervention specification, and treatment fidelity in assistive technology outcomes research. Assist Technol 22(3): 129-138.
- Boger J, Jutai J, Moorhead A, Mulvenna M, Bond R (2019) Ethical Issues in Technology for Dementia. In Using Technology in Dementia Care: A Guide to Technology Solutions for Everyday Living: 43-66.
- de Jesus Alves AC, Matsukura TS (2016) Theoretic models for recommendation and implementation of assistive technology. Cadernos de Terapia Ocupacional da UFS Car 24(3): 591-599.