


Hedayatullah Nayab1, Naseer Ahmad Shinwari2*, Nooria Alikozai3, Ahmadzia Sekandari4, Safiullah Sahebi5, Nabila Naikpai6, Naweed Hassanzada7
1Member of the Dental Department at FMIC hospital, Kabul Afghanistan.
2Research Director and Faculty Member Department of Microbial Technology and Microbiology, Bayazid Rokhan Institute of Higher Education, Kabul, Afghanistan.
3Head of Dental department at FMIC Hospital.
4Dental Consultant at FMIC Hospital.
5Dental Specialist.
6Dental Specialist.
7Dental Trainee at FMIC Hospital.
*Corresponding Author: Naseer Ahmad Shinwari, Research Director and Faculty Member Department of Microbial Technology and Microbiology, Bayazid Rokhan Institute of Higher Education, Kabul, Afghanistan.
Abstract
Introduction: Dental caries in the first permanent molar is the most common disease because they are the first permanent erupting teeth; due to lack of knowledge, people consider it as deciduous teeth, which are not, and most teenagers lose their first permanent molar, which is undeniably the essential unit of mastication, the loss of a first permanent molar in a child can lead to changes in the dental arches that can be traced throughout the life of that person, Dental caries has a significant impact on the general health and development of children it is now well established that oral health is an essential component in defining overall health and quality of life.
Objective: The study aimed to upgrade people's knowledge regarding the importance of teeth maintenance and their first permanent molars. Moreover, the prevalence of dental caries among youths aged 7 to 18 years old determines the vulnerable age.
Method: This observational study included 213 children aged 7 to 18 attending dental check-ups from 06/February/2023 to 31/May/2023. The dental check-up was done with single-use kits, and a toothbrush and tube of toothpaste were gifted to each of them.
Results: According to our survey of 213 patients, 124 patients had dental caries on the first permanent molar. From 213 patients, 108 were girls, and 105 were boys. Of 124 patients with dental caries on the first permanent molar, 68 were girls, and 56 were boys. 59 patients aged 7-12 years and 65 patients aged 13-18 years.
Conclusion: More than half of our survey attendees had permanent molar caries; the mentionable point is this: through the check-up program, we taught them when and how to brush, floss, gum massage, and other necessary oral health hygiene tips, which are not only for oral and dental health but also affects the body, in prevalence of dental caries there is no significant unbalancing change between male and female.
Keywords: Prevalence of dental caries in 1st permanent molar, the importance of 1st permanent molars.
Introduction
Throughout the history of man, diseases have come and disappeared. For most of the major diseases, it has been possible to clarify how ease was brought under control. Such means may include a global vaccination program, living conditions with improved nutrition, and non-contaminated drinking water. For other diseases, explaining the reasons for a change may be more challenging. This Is particularly true for diseases with multifactorial backgrounds, like dental caries. During the decades of caries decline, several actions have been taken to control the disease, and the literature describes numerous studies where one or several factors have been evaluated for their impact. Still, it is difficult to get a complete picture of what happened, as the background is so complex, and many factors may have been directly and indirectly involved. Caries is defined as a microbial disease of the calcified tissue of teeth that leads to demineralization of the inorganic components and subsequent breakdown of the organic moieties of enamel and dentine. The word carries is derived from the Latin word `rot` or `decay.` It is akin to the Greek word `Ker,` meaning death. Fossil teeth accurately record man's state of dentation through the ages. Evidence for caries has been found in homo sapiens since Paleolithic times. Numerous references to dental caries, including early theories attempting to explain its etiology, have been found in the recorded history of ancient people.
A brief review of the history and early theories of the etiology of caries provides an exciting background for understanding the current concept of dental caries. We screened 15,611 AI/AN children in 186 schools. The percentage with four erupted first molars was 27 percent of kindergarten, 76 percent of first, 96 percent of second, and 99 percent of third-grade children. About 7 percent of kindergarteners had decayed, missing, or filled molars compared with 20 percent, 30 percent, and 38 percent of first, second, and third graders, respectively [1] Consumption frequency of added sugars was associated with dental caries some of child demographic and lifestyle characteristics. Children who consume foods and drinks with added sugar more frequently are more likely to develop dental caries, but higher consumption frequency of drinking water in fluoridated areas might reduce dental caries. The findings add to the evidence for the association between children's dental caries and added sugar consumption [2] Prevalence Dental caries in Iceland, During the last decades, a continuous decrease in dental caries has been observed among school children in Iceland. Although sugar consumption increased during this period, especially in the form of sweets and soft drinks, the import of toothpaste increased, and preventive measures such as fissure sealants and fluoride rinsing programs were also intensified. Other factors likely impacted were changes in treatment philosophy and increased personal resources. No single factor is responsible for the onset of the caries decline. Instead, this was a multifactorial effect due to a few different measures.
Prevalence of caries in children and adolescents in Sweden: the prevalence of caries among 3,6, 12, and 9-year-olds in Sweden was followed during 1985-94 through country council reports to the National Board of Health and Welfare. For the age groups studied, the prevalence of caries diminished markedly during the period. The proportion of caries-free 3 and 6 years olds increased. DFT for 12-year-olds sank from 3.1 to 1.5 during 1985-1994; for 19-year-olds, DFT changed from 8.5 to 5.2; this change was attributed to the change in oral hygiene due to better oral prophylaxis. Caries prevalence in Japan: In Japan, the mean DMFT at 12 years of age increased from 2.8 to 5.9 in 1975, but it decreased again to 3.64 in 1993. The increase in caries prevalence can, without doubt, be explained by an increment in sugar consumption, since the intake of sugar increased after World War Two.
On the other hand, the reason why the DMFT has decreased since 1981 needs to be clarified. In many industrialized countries, a caries reduction has been achieved with acceptable fluoride exposure, although sugar consumption was still high. However, fluoride usage was still limited during the last 2 decades in Japan. There is no community where fluoridated drinking water has been supplied since 1972. Fluoride tablet use was also discontinued for children in the 1970s, and fluoride mouth rinsing programs were available for only 1% of school children in 1992. Changes in caries prevalence among adolescents in Germany The post-war increase in total sugar consumption increased caries prevalence among adolescents in both East and West Germany until 1970. The interdiction of fluoridated toothpaste after 1973 in West Germany was followed by caries decline in children and adolescents from very high caries levels of 8.8 DMFT to moderate levels of 5.1 DMFT; other reasons quoted are group prevention, which included fluoride varnish programs and interdiction of free prevention (brushing instructions, fluoridation and sealant) at private dentists for 6-19 years olds since 1983.
Some of the reasons for global decline in dental caries can be summarized as:
1. The widespread use of fluoride toothpaste.
2. Fluoride tablets and fluoride gels.
3. Fluoride rinsing programs.
4. Dietary fluoride supplements.
5. Increased dental awareness.
6. Availability of dental resources.
7. Decrease in sugar consumption.
8. Dental health education programs.
9. Oral prophylaxis.
10. Fissure sealants.
11. Preventive approach in practice.
12. The widespread use of antibiotics.
13. Changes in diagnostic criteria.
14. Herd immunity.
15. As-yet-unknown factors.
Based on the existing data, nearly 60% of Pakistanis have dental caries; the proportion is almost the same in all provinces [3]. The caries prevalence of primary teeth, permanent teeth, and whole dentition (mix of immediate and permanent teeth) among children in Iran was 75.3%, 41.1%, and 89.8%, respectively [4]. In India, the prevalence of dental caries was 54.16%, whereas age-specific prevalence was 62% in patients above 18 years and 52% among 3–18 years of age. Maximum overall prevalence was noted in mixed dentition (58%). Region-wise prevalence was higher in western India (72%). The use of decayed, missed, and filled teeth as diagnostic criteria for early childhood caries was only 29% [5] in Saudi Arabia. The summary estimate of dental caries prevalence among 5- 7-year-old and 12–15-year-old children was 84% and 74%, respectively. Dental caries status among school children is high in SA [6]. Prevalence of dental caries in the first permanent molar and associated risk factors among sixth-grade students in São Tomé Island. This study revealed that the prevalence of dental caries, a common public health problem, was considerably high. The DMFT and DMFS of the first permanent molar were 1.751 ± 1.514 and 3.542 ± 3.941, respectively [7]. Caries Experience in Primary and Permanent Dentition in Children Up to 15 Years of Age from Bosnia and Herzegovina: The permanent teeth sample consists of 242 (49.1%) female and 251 (50.9%) male examinees. There were overall 213 (87.7%) female and 259 (90.2%) male examinees with decayed missing filled teeth-DMFT1≤ and 147 (60.7%) and 152 (60.6%) with Decayed Missing Filled Teeth [8] and in Afghanistan, 213 persons 89 persons had no dental caries on their first permanent molar but unfortunately 124 of them had caries on their first permanent molar, the 105 male from 213 and 60 males had caries and 45 males were clear on the other hand form 108 females 64 of them had caries and 44 of them had no caries on their first permanent molars and 109 between the age 7 to 12 years which 59 of them had caries on first permanent molar and 50 of them had no caries and 104 male and female between the age 13 to 18 years old which 31 person had no caries on the first permanent molar but 73 of them both male and female from 104 people had caries on a first permanent molar).
Symptoms the symptoms of dental caries are the same, such as toothache, continuous pain keeping you awake or occasional sharp pain without an apparent cause, and tooth sensitivity. You may feel tenderness or pain when eating or drinking something hot, cold, or sweet, and grey, brown, or black spots appear on your teeth, as well as gum inflammation and bad breath.
Diagnosis (Dental caries is diagnosed through clinical oral examination (dental check-up) and also in radiography is visible; it is the same in the world and Afghanistan)
Treatment (the treatment of dental caries depends on its damage and decay. It can be treated by a simple filling or a direct and indirect pulp cap, or in profound decays; it may need root canal therapy. The method of treatment is also the same in the world and Afghanistan)
Cost of Treatment Worldwide, the costs of root canal therapy are incompatible, depending on facilities, doctors, or health providers’ personal experience, knowledge, degree, and skills. In Afghanistan, the price is approximately similar to that of regional countries. However, the prices are incompatible with modern European and American countries. For instance, I made a chart of prices from different countries.
|
COUNTRY |
Approximate cost |
COUNTRY |
Approximate cost |
|
United States |
600$ to 1,500$ |
Colombia |
Almost 110$ |
|
Canada |
Almost 1,500$ |
Costa Rica |
Almost 250$ |
|
Australia |
Almost 2,500$ |
Thailand |
Almost 180$ |
|
New Zealand |
Almost 2,000$ |
Cambodia |
Almost 100$ |
|
United Kingdom |
Almost 1,600$ |
Vietnam |
Almost 50$ |
|
Germany |
360 to 440$ |
India |
18 to 150$ |
|
South Korea |
199 to 2000$ |
Afghanistan |
15 to 80$ |
|
Iran |
100 to 200$ |
Pakistan |
27 to 52$ |
Prevention in modern countries they control the diet and even contain the minerals in the water to be within the range of body requirements; the way to prevent caries and important oral hygiene issues are taught to parents during the mother’s pregnancy and also from elementary school (grades K/1) or nursery cycle highly focusing on hygiene and especially oral health information and a regular dental check-up is most beneficial to prevent. Also, it has informative aspects to show the importance of teeth. In addition to dental visits, doctors guide the child on how and when to brush, floss, and other oral hygiene awareness; however, in Afghanistan, there is no strategy for water mineralization, and poverty causes malnutrition. Of the high percentage of illiteracy in Afghanistan, about 45.85% of the population is illiterate.
Objectives
This study aims to estimate the prevalence of dental caries among teenagers in Kabul, Afghanistan, to measure the incidence of dental caries among teenagers aged 7–18 years to find in which years the teenagers are most vulnerable to dental caries. Knowledge increment: besides our dental check-up during the study, we had a knowledge improvement program for participants, including teenagers and their parents or other family members, regarding the importance of oral and dental hygiene, concerning different methods to improve their health through healthy mouth and teeth.
Methodology
Study design: An observational Study
Participants: In this survey, we observed 213 patients, both males and females, in France Medical International Centre, Kabul, Afghanistan, who came to the dental department.
Sample taking: All patients with dental caries from the beginning of January 2023- August 2023 that we saw and registered in the register books of FMIC, and the sample of the Research was done by taking samples from the same register and patients' files.
Inclusion criteria: All patients who had the clinical evidence of the dental caries and had completed the necessary examinations available in the dental department of FMIC, and in addition to their complementary reputation, their registry and case file included my Research.
Exclusion criteria: Those who didn’t meet the above criteria were not included in my Research. Like dental calculus, gingivitis, dental caries on deciduous teeth for those under the age of 12 years.
Data collection: Collecting data from the books of the dental department of FMIC register, clinic, and patient file was a data collection form; this data form includes serial number, registration number, patient age, patient sex, and patient residence.
Data analysis: SPSS was used to analyze patients’ data according to the data collection form.
Results
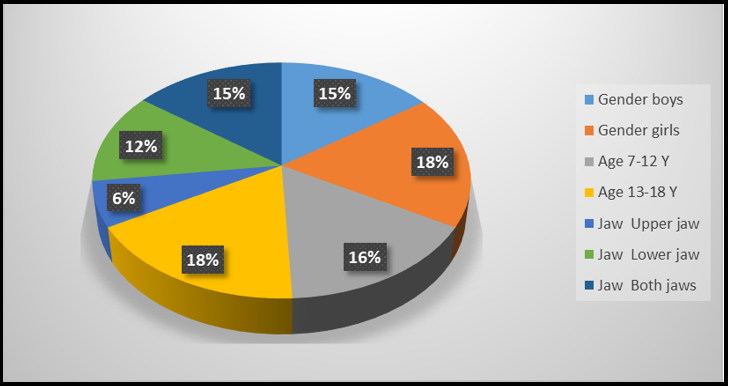
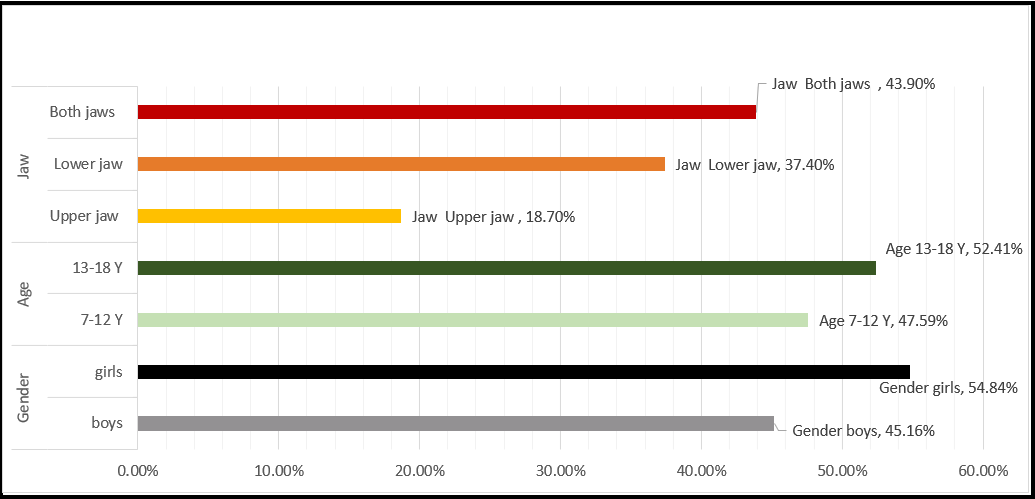
Regarding our survey of 213 persons that we checked their teeth, 124 persons (58.1%) had dental caries on the first permanent molar; fortunately 89 persons almost (41,9%) had no dental caries on the first permanent molar, 105 attendees (49%) were males, and 108 (51%) were females, 60 boys (48%) had first molar caries, and almost 64 girls (52%) had first permanent molar caries it means that there is no significant difference in the prevalence of caries on first permanent molar between male and female .109 children of the survey were between 7 to 12 years old 59 children (54%) of 109 children aged 7 to 12 years had caries on first permanent molar and 104 attendees were 12 to 18 years old that 73 people (70%) of 104 people aged 13 to 18 years old had caries on their first permanent molar caries it shows that prevalence of caries is more common at the age of 13 to 18 than 7 to 12 years, shown in the bellow table.
|
Variables |
|
Percentage |
Frequency |
|
Gender |
boys |
45.16% |
56 |
|
|
girls |
54.84% |
68 |
|
Age |
7-12 |
47.59% |
59 |
|
|
13-18 |
52.41% |
65 |
|
Jaw |
Upper jaw |
18.7% |
23 |
|
|
Lower jaw |
37.4% |
47 |
|
|
Both jaws |
43.9% |
54 |
Discussion
The current concept of dental caries in the epidemiological model, a disease state is due to the interplay of three primary factors (Keyes and Jordan,1960): the host, the agent or recruiting factors, and environmental influence (tooth, substrate, flora) new-burn in 1982 postulated that many secondary factors (PH composition, saliva, flow rate PH, bullrings capacity) also influence the rate of progression of caries between three primary factors is essential for the initiation and progression of caries, Dental caries remains one of the most wide-spread diseases of humanity. Advances in prophylactic measures to deal with this disease have significantly reduced the overall caries rate. However, the Surgeon General’s 2000 report on oral health in America stated that most five to nine-year-old children have at least one lesion on their teeth. This percentage increases to 84.7% in adults at least 18 years of age. In developing countries, dental caries are often at epidemic proportions, especially among people with low incomes. A landmark experiment in the 1960s established that mutans streptococci are the primary etiologic agents of the disease and that this infection is transmissible.
A strong association exists between the level of colonization with mutants streptococci and dental caries, although other organisms, such as lactobacilli, have also been implicated in this disease. Salivary gland pathologies also increase dental caries due to xerostomia; xerostomia refers to a subjective sensation of a dry mouth; it is frequently, but not always, associated with salivary gland hypo-function causes of xerostomia can be developmental like salivary gland aplasia, iatrogenic such as medication, radiation therapy to the head and neck, systemic disease HIV infection psychogenic, or local factors like decreased mastication and mouth breading. Dental caries are a concerning issue because they are common among children and negatively impact their quality of life. Caries is a global public health challenge that is continuously studied and documented in various countries. In 2020, the global prevalence of dental caries in primary and permanent teeth was estimated at 46.2 and 53.8%, respectively, which was considered high. Enamel and dentine crystals are tiny, 40 nm and 10 nm in diameter, respectively. They are comprised of a hydroxyapatite-like mineral that contains many impurities and inclusions of other ions that cause the mineral of enamel and dentine to be much more soluble than pure hydroxyapatite or Fluorapatite. The primary inclusion that makes dental minerals much more acid soluble than hydroxyapatite or Fluorapatite is the carbonate ion that substitutes for the phosphate ion in the crystal lattice, producing defects and calcium-deficient regions.
Approximately 1 out of 10 phosphate ions in enamel are replaced by carbonate and 1 out of 5 in dentine. Demineralization occurs in two steps. First, the bacteria metabolize fermentable carbohydrates, producing organic acids that diffuse into the tooth through the water amongst the crystals. When the acid reaches a susceptible site on a crystal surface, calcium and phosphate are dissolved into the surrounding aqueous phase between the crystals. It is a high-resolution electron micrograph of a single crystal from a region of sound enamel. His technique only visualizes the electron-dense calcium ions that appear as straight rows of dots derived from calcium ions. Phosphate, hydroxyl, and fluoride ions cannot be seen with this technique. The white patches are regions of calcium deficiency that are most susceptible to acid attack because of the substitution of phosphate ions by carbonate ions during tooth and bone development. That shows two crystals from the body of a natural carious lesion. The small calcium-deficient defect areas visualized have expanded into hexagonal-shaped regions where the mineral has dissolved during an acid attack. This is the first stage of Demineralization occurring at the atomic level far before it can be seen visually as gross Demineralization. This is the first step in the dental caries process continuum, which can eventually lead to cavitation.
Dental caries is the localized destruction of susceptible dental hard tissues by acidic by-products from bacterial fermentation of dietary carbohydrates.[4,6] The signs of this Demineralization are seen on the hard dental tissues, but the disease process is initiated within the bacterial biofilm (dental plaque) that covers a tooth surface. Moreover, the very early changes in the enamel are not detected with traditional clinical and radiographic methods. Dental caries is a multifactorial disease that starts with microbiological shifts within the complex biofilm and is affected by salivary flow and composition, exposure to fluoride, consumption of dietary sugars, and creative behaviors (cleaning teeth). The disease is initially reversible and can be halted at any stage, even when some dentine or enamel is destroyed (cavitation), provided enough biofilm can be removed. Dental caries is a chronic disease that progresses slowly in most people. The disease can be seen in both the crown (coronal caries) and root (root caries) portions of primary and permanent teeth and on smooth, pitted, and fissured surfaces. It can affect the enamel, the outer covering of the crown; cementum, the outermost layer of the root; and dentine, the tissue beneath both enamel and cementum. Caries in the primary teeth of preschool children are commonly referred to as early childhood caries.
Global decline in dental caries
Several excellent reviews have been published in recent years, and there is a general agreement that a marked reduction in caries prevalence has occurred among children in most industrialized countries. This is true for countries using water fluoridation as a preventive measure and for countries without such programs. Some of the factors in caries decline are such as
1. Diet
A. Improved nutrition.
B. Decrease in amount t of sugar consumption.
C. Reduce the frequency of sugar consumption.
D. Use of sugar substitute.
2. Fluoride
A. Water fluoridation.
B. Fluoride toothpaste.
C. Fluoride tablets.
D. Fluoride school programs.
E. Fluoride application by dentist.
3. Plaque
A. Reduce plaque due to better brushing habits.
B. Better chemical plaque control.
C. Flossing of interproximal.
4. Miscellaneous
A. Pit and fissure sealants.
B. Saliva.
Histopathology of dental caries
As the carious lesion invades the dentine, the dentinal tubules become involved. This is divided into five zones, proceeding from the lesion inward to the normal dentine
1. Zone of decomposed dentine.
2. Zone of bacterial invasion.
3. Zone of Demineralization.
4. Zone of dentinal sclerosis.
5. Zone of fatty degeneration.
These zones are only discrete and distinguishable as separate entities in slowly advancing carious lesions and are probably passive changes imparted on the dentine by the invading microorganisms, including their indirect effect due to Demineralization.
Diet And Dental Caries
Our diet habits have undergone considerable changes in quantity and quality since our evolution. Food can have a two-fold effect because the effects of nutrition are mediated systemically, and the effects of diet are manifested locally. The relationship between diet and tooth is of great importance regarding tooth decay. Microorganisms are heavily responsible for caries, but the significance of the substrate must be supported because microorganisms can only cause caries with a suitable substrate. The occurrence of caries depended on two factors - pre-eruptive (blood, saliva) and post-eruptive actors (maturation, mineralization, chelation, plaque, bacteria).
Conclusion
Dental caries of the first permanent molar are more common at 13 to 18 than at 7 to 12. It shows that after the eruption of the first permanent molar due to carelessness, as the age goes higher, the risk of caries also increases, and there is no significant difference in gender.
Ethical Approval
This study was ethically approved by the medical bioethics committee of the BRIHE ethics committee (Code: BRIHE-1394-1402). The patients/participants provided their written informed consent to participate in this study.
Strengths:
1. The study is based on a large sample size, as it includes both teenage boys and girls.
2. The research is conducted at FMIC Hospital, which is a reputable and well-known healthcare facility in Kabul, Afghanistan. Therefore, the data collected can be considered reliable and representative of the population in that region.
3. The study design is Observational, allowing for data to be in a hospital setting, which may provide a more accurate representation of the prevalence of dental caries compared to community-based studies.
4. The study design is an observational study, that allows for examining dental caries at a specific point in time, providing valuable information on the current state of dental health among teenage boys and girls.
Limitations:
1.The study is conducted in a single hospital in Kabul, Afghanistan, which may limit the generalizability of the findings to other populations or regions.
2.Being a cross-sectional study, it only provides a snapshot of the prevalence of dental caries at one point in time and does not allow for the assessment of trends or causality.
3.The study relies on self-reporting or clinical examination for the diagnosis of dental caries, which may introduce measurement bias and inaccuracies.
4.There may be confounding factors that were not considered or controlled for in the study, such as dietary habits, oral hygiene practices, or socio-economic status, which could influence the prevalence of dental caries.
5.The study does not provide information about the severity or treatment status of dental caries, limiting the understanding of the overall impact on oral health.
References
- Phipps KR, Ricks TL, Blahut P (2013) Permanent first molar eruption and caries patterns in American Indian and Alaska Native children: challenging the concept of targeting second grade for school-based sealant programs. J Public Health Dent. 73(3): 175-8.
- Hong J, Whelton H, Douglas G, Kang J (2018) Consumption frequency of added sugars and UK children's dental caries. Community Dent Oral Epidemiol. 46(5): 457-464.
- Siddiqui AA, Alshammary F, Mulla M, Al-Zubaidi SM, Afroze E, et al. (2021) Prevalence of dental caries in Pakistan: a systematic review and meta-analysis. BMC Oral Health. 21(1): 450.
- Soltani MR, Sayadizadeh M, Raeisi Estabragh S, Ghannadan K, Malek-Mohammadi M (2020) Dental Caries Status and its Related Factors in Iran: A Meta-Analysis. J Dent (Shiraz). 21(3): 158-176.
- Balaji SM (2018) Dental caries: Research perspective. Indian J Dent Res. 29(1): 3.
- Alshammari FR, Alamri H, Aljohani M, Sabbah W, O'Malley L, et al. (2021) Dental caries in Saudi Arabia: A systematic review. J Taibah Univ Med Sci. 16(5): 643-656.
- Que L, Jia M, You Z, Jiang LC, Yang CG, et al. (2021) Prevalence of dental caries in the first permanent molar and associated risk factors among sixth-grade students in São Tomé Island. BMC Oral Health. 21(1): 483.
- Obradović M, Dolić O, Milovanović V, Karaman N, Mišić M, et al. (2023) Caries Experience in Primary and Permanent Dentition in Children Up to 15 Years of Age from Bosnia and Herzegovina- A Retrospective Study. Children (Basel). 10(4): 754.