


Dakotah Weaver, Amanda C Philp*, Kristin Hanson
The Chicago School of Professional Psychology, Applied Behavior Analysis Department, Chicago, IL, USA
*Corresponding Author: Amanda C Philp, The Chicago School of Professional Psychology, Applied Behavior Analysis Department, Chicago, IL, USA
Abstract
This case study applied a functional behavior assessment (FBA) methodology to thumb-sucking exhibited by a 5-year-old girl with Autism Spectrum Disorder (ASD). Results from the FBA indicated thumb-sucking to be high frequency and across assessment conditions for the client. The authors used the FBA data to guide intervention development and implementation. The intervention included Differential Reinforcement of Other Behavior (DRO) combined with a response blocking procedure (thumb guard) to reduce thumb-sucking. Following intervention implementation, thumb-sucking decreased, as evidence by the decrease in the frequency of the behavior. We also discuss the results in terms of the intervention's effectiveness.
Keywords: differential reinforcement, response blocking, thumb-sucking, thumb guard
Introduction
Thumb-sucking is an adaptive and normative behavior that may emerge in early childhood. However, when thumb-sucking persists into later childhood, it can lead to socially significant and/or medical problems. In some children, chronic thumb-sucking may require treatment. Thumb-sucking is estimated to occur in up to 73 % of children between 2 and 5 years (Borrie et al., 2015). As children grow older, the behavior tends to stop; however, this behavior persists in 1.9 % of 12-year-old children (Borrie et al., 2015). Thumb-sucking is a behavioral habit that is categorized as non-nutritive sucking habits (Borrie et al., 2015; Staufert-Gutierrez & Carugno, 2020). Practitioners must be aware of the non-nutritive sucking habits and their negative impacts on oral health and the complications that can arise with them (Friman, 1987; Luke & Howard, 1983; Nasir & Nasir, 2015, Reid & Price, 1984; Schmitt, 1987). If thumb-sucking continues into late childhood, negative consequences can occur. For example, a deformity of the nail, dental malocclusion, digital deformities, speech difficulties, or paronychia may occur (Nasir & Nasir, 2015). The behavior of thumb-sucking can be addressed with different interventions, from fitting a dental appliance, parental and patient advice, or behavior modification techniques such as response blocking and positive reinforcement (Ellingson et al., 2000; Friman & Hove, 1987; Stricker et al., 2001; VanHouten & Rolider, 1984). From a behavioral perspective, habits are learned operations maintained by positive, negative, or automatic reinforcement (Watson & Dufrene, 2004). Positive reinforcement is defined as the occurrence of behavior followed immediately by the presentation of a stimulus that increases the future frequency of the action in similar situations (Cooper et al., 2019). There are several variations of positive reinforcement called differential reinforcement. Differential reinforcement of other behaviors (DRO) is a reinforcement procedure in which reinforcement is delivered for any response other than a specific target behavior (Cooper et al., 2019). This procedure decreases a particular target behavior because it is never followed by reinforcement; thus, it weakens the future rate. Another technique that reduces behaviors is called response blocking. Response blocking refers to physically preventing an action from occurring. Typically, a visible motor response is required for a response blocking intervention. Since motor behaviors are maintained by automatic reinforcement, response blocking is an effective intervention (Cooper et al., 2019). One way to determine the function of a behavior is through a functional behavior assessment (FBA). An FBA provides a promising approach for identifying environment al determinants for a habit, but the data can also be used to inform intervention and treatment planning (Watson et al., 2005; Woods et al., 2001).
There is little research on the treatment of thumb-sucking using behavior modification approaches. Preliminary research on reducing thumb-sucking using either positive reinforcement or punishment was conducted over 20 years ago with little updated research. To date, only a few studies have attempted to gain information regarding the functions of digit (finger or thumb) sucking behaviors. For example, (Miltenberger et al. (1998) conducted a functional analysis of the thumb sucking of a 7-year-old girl. They found that the behavior was most evident in the alone condition. Similarly, (Rapp et al. (1999) assessed thumb sucking that was exhibited by a 5-year-old boy. Their results determined that the behavior was maintained in the absence of social consequences.
The purpose of the present case study was two-fold, first to identify the function of thumb-sucking for the client, then assess the direct effects of response blocking via protective equipment (e.g., thumb guards) with a differential reinforcement of other behavior (DRO) intervention.
Methods
Participant and Setting
MaTi was a five-year-old girl with a medical diagnosis of autism and SLC6A (a rare genetic disorder). MaTi attended a small private clinical setting that employed applied behavior analysis services. All assessments and interventions sessions were conducted in the clinic, and sessions were three hours in length daily.
Response Measurement and Interobserver Agreement
The target response was thumb-sucking. Thumb-sucking was defined as any instance of inserting thumb into mouth past the lips' plan for at least 1 s. Thumb-sucking cases were separated by at least 2 s. Frequency data were collected during each phase. A plus (+) was recorded for each instance of behavior. The data was then summed at the end of the session and graphed a total sum for the day.
Interobserver agreement (IOA) was collected by having a second independent observer record data. The agreement was calculated by dividing the lesser total count by the greater total count and multiplying by 100 %. IOA was scored across three sessions with 100 % agreement. Treatment integrity, the degree to which the intervention is being implemented as written, was also calculated. Treatment integrity was 100 % and taken on 33 % of random sessions and included at least one session from each condition.
Procedure
Before the study, MaTi's parents were interviewed. The interview revealed that throughout the day, MaTi would engage in a high rate of thumb-sucking. Subsequently, a functional behavior assessment (FBA) was conducted for thumb-sucking to determine the variables that maintained it. Data were collected on the antecedent and consequences that immediately proceeded before the behavior and after the behavior. The observer recorded all behavior instances using anecdotal notes of the events.
The results of the FBA indicated that thumb-sucking was automatically reinforced. Therefore, a combination of interventions that entailed DRO and response blocking was decided upon with parental consent. During the intervention, there were four different phases and nine sub-phases, Appendix A. The phases were to get MaTi used to wearing the guards and then systematically fade the guards' wearing over the phases. The sub-phases were utilized for different intervals to tell the researchers how long MaTi had to go before getting reinforcement. Refer to Appendix A for detailed steps of the intervention across phases and sub-phases.
Results
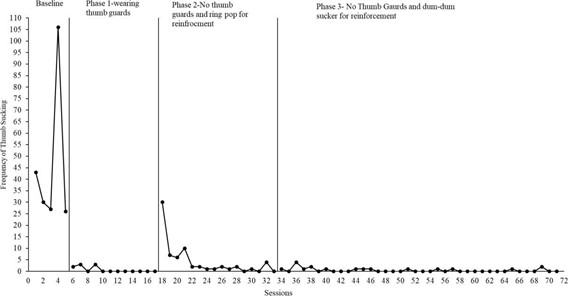
Results of the intervention is found in Figure 1. During the baseline condition, the mean frequency of thumb-sucking was 46.4 (range 26- 106). During the first phase of intervention (wearing the thumb guard with access to reinforcement), the mean frequency of thumb-sucking decreased to 0.67 (range 0-3). For the second phase (not wearing Figure 1: Frequency of thumb sucking across intervention phases thumb guards with access to reinforcement), mastery of the step took 16 sessions, with the mean frequency of 4.31 (range 0-30). In phase three (not wearing thumb guard and shift of reinforcement), the mean frequency was 0.56 (range 0-4), Figure 1. Results of thumb-sucking dramatically decreased from baseline through all intervention phases.
Discussion
The results of the FBA showed that the maintaining function of thumb-sucking was automatic reinforcement. In order to treat the automatically maintained thumb-sucking, a DRO procedure plus response blocking via a thumb guard was implemented. The intervention results revealed that the combination of a DRO procedure with response blocking effectively reduced thumb-sucking frequency in the child. In baseline MaTi, on average, had 46.4 instances of thumb-sucking; however, at the conclusion of phase 3, that frequency went down to an average of 0.56, with four instances being the max number of thumb-sucking in three hours. The thumb guards blocked the response and prevented MaTi from getting reinforcing consequences from sucking her thumb.
For MaTi, we hypothesized that the elimination of thumb-sucking that was produced throughout the glove a fading period is most likely attributable to sensory extinction (Iwata et al., 1994). That is, the guard's use prevented the production of stimulation and oral stimulation from thumb-sucking, resulting in the elimination of the behavior. Although sensory extinction seems the most likely process accounting for eliminating thumb-sucking for MaTi, it is also possible that the gloves produced an aversive taste, thus punishing finger sucking (Mazaleski et al., 1994).
The results of this investigation extend the current literature on digit sucking (e.g., fingers and/or thumb) in several ways. First, this is one of only a few studies that have attempted to identify the function of finger or thumb sucking (Miltenberger et al., 1998; Rapp et al., 1999). Consistent with previous studies (Kennedy & Souza, 1995; Piazza et al., 1996; Rapp et al., 1999), analyses were conducted to identify sensory consequences maintaining the behavior (i.e., digital, oral, or both). Last, this study is the first to evaluate the fading of a sensory attenuation device (i.e., the glove) in a child with autism. Because both of these interventions reduce behavior in the absence of socially mediated consequences, additional research with these procedures is warranted.
Some limitations of this study should be acknowledged. First, this study was conducted during COVID-19. Therefore, the Center for Disease Control precautions were in place, which limited the participants and forced the researchers to wear face coverings. Unfortunately, socially distancing was not maintained between the client and adults. Second, conclusions regarding the specific sensory consequences that maintained MaTi's behavior could not be reached through the FBA. The results of this study provide several avenues for future investigations in the analysis and treatment of behavior maintained by sensory reinforcement. First, future research should continue to extend functional analysis methods for automatically reinforced behavior. Second, we eliminated MaTi's thumb-sucking over several months and faded use of the guard in the clinic. Future research should focus on determining the minimum amount of time necessary to extinguish this behavior to complete the attenuation procedure promptly. Also, because it is difficult to discriminate between the behavior change produced by reinforcer competition and reinforcer substitutability, researchers should continue to use methods to attenuate the stimulation produced by behavior maintained in the absence of socially mediated consequences. Finally, due to the immediate reduction in behavior produced with the DRO/response blocking and the parent's high acceptability ratings, further evaluation of the intervention should be generalized across multiple settings.
Conflict of interest: We have no known conflict of interest to disclose.
Funding: No funding was utilized for this study.
References
- Borrie FR, Bearn DR, Innes NP, Iheozor-Ejiofor Z (2015) Interventions for the cessation of non-nutritive sucking habits in children. The Cochrane database of systematic reviews, (3): CD008694.
- Cooper J, Heron T, Heward W (2019) Applied Behavior Analysis (3rd Edition). Hoboken, NJ: Pearson Education.
- Ellingson SA, Miltenberger RG, Strieker JM, Garlinghouse MA, Roberts J, et al. (2000). Analysis and treatment of finger sucking. Journal of Applied Behavior Analysis. 33: 41-52.
- Friman PC (1987) Thumb sucking in childhood. Feelings and their medical significance, 29, 11-14.
- Friman PC, Hove G (1987) Apparent covariation between child habit disorders: Effects of successful treatment for thumb sucking on untargeted chronic hair pulling. Journal of Applied Behavior Analysis. 20(4): 421-425.
- Iwata BA, Pace GM, Cowdery GE, Miltenberger RG (1994) What makes extinction work: Analysis of procedural form and function. Journal of Applied Behavior Analysis. 27(1): 131-144.
- Kennedy CH, Souza G (1995) Functional analysis and treatment of eye poking. Journal of Applied Behavior Analysis. 28(1): 27- 37.
- Kumar V, Shivanna V, Kopuri RC (2019) Knowledge and attitude of pediatricians toward digit sucking habit in children. Journal of the Indian Society of Pedodontics and Preventive Dentistry, 37(1): 18–24.
- Luke LS, Howard L (1983) The effects of thumb sucking on orofacial structures and speech: A review. The compendium of continuing education. 4(6): 575-579.
- Mazaleski JL, Iwata BA, Rodgers TA, Vollmer TR, Zarcone JR (1994) Protective equipment as treatment for stereotypic han mouthing: Sensory extinction or punishment effects? Journal of Applied Behavior Analysis. 27(2): 345-355.
- Miltenberger RG, Long ES, Rapp JT, Lumley V, Elliot AJ (1998) Evaluating the function of hair pulling: A preliminary investigation. Behavior Therapy. 29(2): 211-219.
- Nasir A, Nasir L (2015) Counseling on Early Childhood Concerns: Sleep Issues, Thumb-Sucking, Picky Eating, School Readiness, and Oral Health. American family physician. 92(4): 274–278.
- Piazza CC, Hanley GP, Fisher W (1996) Functional analysis and treatment of cigarette pica. Journal of Applied Behavior Analysis. 29(4): 437-450.
- Rapp JT, Miltenberger RG, Galensky T, Roberts J, Ellingson SA (1999) Brief functional analysis and simplified habit reversal treatment of thumb sucking in fraternal twin brothers. Child and Family Behavior Therapy. 21(2): 1-17.
- Reid DA, Price AH (1984) Digital deformities and dental malocclusion due to finger sucking. British journal of plastic surgery. 37(4): 445-452.
- Schmitt BD (1987) Your child's health. Bantam: Toronto.
- Staufert-Gutierrez D, Carugno P (2020) Thumb Sucking. StatPearls. Treasure Island: Florida.
- Stricker JM, Miltenberger RG, Garlinghouse MA, Deaver CM, Anderson CF (2001) Evaluation of an awareness enhancement device for the treatment of thumb sucking in children. Journal of Applied Behavior Analysis. 34(1): 77-80.
- VanHouten RV, Rolider A (1984) The use of response prevention to eliminate nocturnal thumb sucking. Journal of Applied Behavior Analysis. 17(4): 509-520.
- Watson TS, Dufrene BA (2003) An evaluation of a brief functional analysis format within a vocational setting. Journal of Applied Behavior Analysis. 36(1): 125-128.
- Watson TS, Dufrene BA, Weaver AD, Butler T, Meeks C (2005) Brief antecedent assessment and treatment of tics in the regular education classroom: A preliminary investigation. Behavior Modification, 29(6): 839-857.
Appendix A
Phase 1: The goal is for MaTi to decrease the frequency of thumb sucking to 0 instances for the entire duration of the session (3 hrs.) - DRO Ring pop + Intervention with guard
- Instruct MaTi to put on her thumb guards on each hand (if not already wearing them when she arrives).
- The therapist will wear a timer, and have it set to duration according to the current sub-phase. MaTi must keep guards on and have zero instances of thumb sucking for the full duration in order to receive reinforcement (ring pop). A sub-phase will be considered mastered once Malia has 2 consecutive data points with 0 instances of thumb sucking. Therapist will have ring pop open and ready in a bowl out of reach of MaTi (on top of the cabinet in a room). *MaTi is not allowed access to Ring Pop (or any sucker) any other the time during the session.
- Phase 1a – 5 min (30-sec access to ring pop)
- Phase 1b – 15 min (30-sec access to ring pop)
- Phase 1c – 30 min (30-sec access to ring pop)
- Phase 1d – 45 min (30-sec access to ring pop)
- Phase 1e – 60 min (30-sec access to ring pop)
- Phase 1f – 90 min (30-sec access to ring pop)
- Phase 1g – 2 hr. (2 min access to ring pop)
- Phase 1h - 2.5 hr. (3 min access to ring pop)
- Phase 1i – 3 hr. (4 min access to ring pop)
- Make sure there is a NEW ring pop and CLEAN bowl prior to the start of each session.
- If MaTi takes off her guard OR engages in the thumb sucking, a therapist will reset the time on the timer and start over.
- Every time MaTi goes up to engage in thumb sucking behavior and then DOESN'T therapist will immediately reinforce the client with verbal praise. "Nice job keeping your thumb down"
- If MaTi goes the entire sub-phase duration without engaging in thumb sucking, reinforce with 30 seconds access to ring pop, and say,
"Nice job keeping your thumb out of your mouth".
- During ring pop reinforcement, a therapist will not interfere with Malia.
- No demand should be placed on MaTi during this time.
- When 30 seconds elapses, a therapist will remove access to ring pop.
- If she asks for more access to the ring pop, a therapist may tell her "you can have more ring pop if you keep your thumb out of your mouth." (Ignore any continued requests).
- Note: bring the bowl with the ring pop with you EVERYWHERE MaTi goes (i.e., wagon rides, bathroom, gym, gameplay, social time with peer, etc.).
Phase 2: The goal is for MaTi to decrease the frequency of thumb sucking to 0 instances for entire duration of a session (3 hrs.) - DRO Ring pop + intervention WITHOUT guards
- MaTi will no longer wear her guards moving forward
- The therapist will have a timer, and have it set to duration according to the current sub-phase. MaTi must have zero instances of thumb sucking for the full duration in order to receive reinforcement (ring pop). A sub-phase will be considered mastered once MaTi has 2 consecutive data points with 0 instances of thumb sucking. The therapist will have ring pop open and ready in a bowl out of reach of MaTi (on top of a cabinet in the room). *Malia is not allowed access to Ring Pop (or any sucker) any other time during the session.
- Phase 2a – 5 min (30-sec access to ring pop)
- Phase 2b – 15 min (1 min access to ring pop)
- Phase 2c – 30 min (1.5 min access to ring pop)
- Phase 2d – 45 min (2 min access to ring pop)
- Phase 2e – 60 min (2.5 min access to ring pop)
- Phase 2f – 90 min (3 min access to ring pop)
- Phase 2g – 2 hr. (3.5 min access to ring pop)
- Phase 2h - 2.5 hr. (4 min access to ring pop)
- Phase 2i – 3 hr. (4.5 min access to ring pop)
- Make sure there is a NEW ring pop and CLEAN bowl prior to the start of each session.
- If MaTi engages in thumb sucking, the Therapist will immediately block and assist MaTi with removing the thumb from the mouth and say, "Thumb stays out of the mouth". The therapist will let MaTi know that the time will now start over. The therapist will reset the time on the timer.
- Every time MaTi goes up to engage in thumb sucking behavior and then DOESN'T therapist will immediately reinforce the client with verbal praise. "Nice job keeping your thumb out of the mouth"
- If MaTi goes the entire sub-phase duration without engaging in thumb sucking, reinforce with Ring Pop, and say, "Nice job keeping your thumb out of your mouth".
- During ring pop reinforcement, a therapist will not interfere with MaTi.
- No demand should be placed on MaTi during this time.
- When the specific time elapses, a therapist will remove access to ring pop.
- If she asks for more access to the ring pop, the therapist may tell her "you can have more ring pop if you keep your thumb out of your mouth." (Ignore any continued requests).
- Note: bring the bowl with the ring pop with you EVERYWHERE MaTi goes (i.e., wagon rides, bathroom, gym, gameplay, social time with peer, etc.).
Phase 3: The goal is for MaTi to decrease the frequency of thumb sucking to 0 instances for entire duration of session (3 hrs.) - DRO Dum Dum Sucker + Intervention (no guards)
- The therapist will have a timer, and have it set to duration according to the current sub-phase. MaTi must have zero instances of thumb sucking for the full duration in order to receive reinforcement (dumb-dumb sucker). A sub-phase will be considered mastered once MaTi has 2 consecutive data points with 0 instances of thumb sucking. Therapist will dum dum sucker pop open and ready in a bowl out of reach of MaTi (on top of a cabinet in the room). *Have extra suckers ready. *MaTi is not allowed access to sucker any other time during the session.
- Phase 3a – 5 min (30-sec access to sucker)
- Phase 3b – 15 min (1 min access to sucker)
- Phase 3c – 30 min (1.5 min access to sucker)
- Phase 3d – 45 min (2 min access to sucker)
- Phase 3e – 60 min (2.5 min access to sucker)
- Phase 3f – 90 min (3 min access to sucker)
- Phase 3g – 2 hr. (3.5 min access to sucker)
- Phase 3h - 2.5 hr. (4 min access to sucker)
- Phase 3i – 3 hr. (4.5 min access to sucker)
- Make sure there is a NEW sucker and CLEAN bowl prior to the start of each session.
- If MaTi engages in thumb sucking, a therapist will reset the time on the timer and start over.
- Every time MaTi goes up to engage in thumb sucking behavior and then DOESN'T therapist will immediately reinforce the client with verbal praise. "Nice job keeping your thumb down"
- If MaTi goes the entire sub-phase duration without engaging in thumb sucking, reinforce with 30 seconds access to sucker, and say, "Nice job keeping your thumb out of your mouth".
- During sucker reinforcement, a therapist will not interfere with MaTi.
- No demand should be placed on MaTi during this time.
- When 30 seconds elapses, the therapist will remove access to sucker.
- If she asks for more access to the sucker, the therapist may tell her "you can have more sucker if you keep your thumb out of your mouth." (Ignore any continued requests).
- Note: bring the bowl with the sucker with you EVERYWHERE MaTi goes (i.e., wagon rides, bathroom, gym, gameplay, social time with peer, etc.).