


Othman MS*, Leong JF, Ong KC, Wan KL, Ahmad Shah SA, Mohd Sofian A, Teo SL, Towil B
Department of Orthopaedic Surgery, Hospital Sungai Buloh, Jalan Hospital 47000 Sungai Buloh, Selangor, Malaysia.
*Corresponding Author: Othman MS, Department of Orthopaedic Surgery, Hospital Sungai Buloh, Jalan Hospital 47000 Sungai Buloh, Selangor, Malaysia.
Abstract
This is a case series of four patients with variety of fractures over malleolar region of the ankle accompanied with either open injuries or poor soft tissue envelopes. These cases were performed in a single centre from February 2019 to February 2020. We used Hybrid Ilizarov External Fixator technique with 2 full rings proximal to fracture’ site and another plantar half ring or foot plate with dorsal foot ring across the ankle. All reduction of articular fragments and alignment of fractures performed via indirect reduction or percutaneously with aid of Image Intensifier. Average time on frame was 14 weeks. All fractures healed without residual infection. Functional outcomes at 1 year are good with AOFAS average score of 82, FADI score of 81 and VAS pain score of 1.4. Despite severe injuries, all patients have stable ankle but suffered from moderate restriction of sagittal motion (flexion plus extension). In summary, the Ilizarov External Fixator technique is a good option of management to be considered for these complex injuries.
Keywords: Ilizarov External Fixator, Malleolar fractures, Ankle fractures.
Introduction
Complex fractures around the ankle region, both closed and open with poor soft tissue envelopes are almost non amenable for conservative management. The daunting complications of malunion and non-union with late sequalae of arthritis are very well known in many cases. The most common advocated pathway is to ‘span, scan and plan’ which subsequently tailoring for delayed internal fixation. This entails the use of plate to obtain optimum stability or minimalist approach of screws and wires plus conventional external fixator to maintain the length. The anticipated problem with massive internal fixation approach would be infection thus risking for further surgical morbidities such as amputation. On the other hand, minimalist approach will render to instability thus risking fixation failure and leading to other complications.
Therefore, the role of Ilizarov External fixator with combined indirect reduction or percutaneous reduction provides alternative option to these horrendous injuries. In general, Ilizarov External Fixator is well known for gradual bone lengthening and transporting bone segment in void area due to resected osteomyelitic bone. However, this apparatus can also be applied successfully and extended its usage in both open and closed fracture management with poor soft tissue envelope. The advantages are vast that include preservation of remaining blood supply through minimal reduction or indirect reduction of fragments that is paramount in fracture healing. Furthermore, the stability of the device itself allows patient to load the fracture site early through weight bearing.
Case Presentation
In overall, cases were divided into closed fracture or open fracture using Tescherne classification or Gustilo classification, respectively. [1,2] Initial treatments includes emergent wound debridement and majority of patient was skeletally stabilised with conventional external fixator. Intervention with Ilizarov External Fixator generally decided once soft tissue was deemed not suitable for internal fixation within 2 weeks post trauma.
Ilizarov External Fixator was either prefabricated preoperatively or constructed progressively during operation with 2 complete rings over the tibia, proximal to fracture site and spanned across the ankle with either a) foot plate and dorsal foot ring or b) plantar half ring and a dorsal foot ring. (Figure 1).
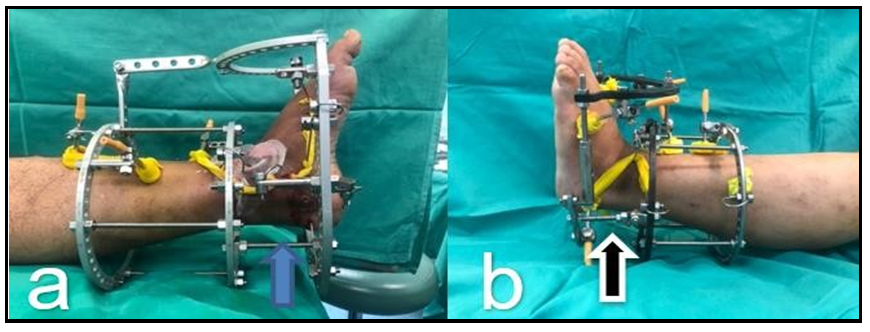
Figure 1: 2 different constructs utilising (a) footplate and dorsal half-ring with straight connection rod (Blue arrow) and (b) plantar and dorsal half rings with hinged connection (black arrow) connecting ankle joint construct
The sequences of operative procedures were as followed: -
1. Fibula length - Intramedullary wire was inserted into fibula fracture to achieve reasonable length
2. Ankle mortise and alignment - Assembly of Ilizarov ring, both on tibial and foot frame construct.
a. In minimal intraarticular injury, the alignment and ankle mortise were adjusted with straight connection rods over both constructs. (Blue arrow on Figure 1)
b. In severe injury including subluxation and dislocation, we used the foot construct as manual traction to disimpact the fracture site before attaching the tibial construct and foot construct using the hinged connecting rod. (Black arrow on Figure 1)
3. Reduction of key fragments
a. Under the image intensifier, olive wires with washers were inserted at the apex of fracture fragments (most obvious bony cortices under Image Intensifier) and connected to adjacent Ilizarov rings (see Figure 2). The use of washers was advocated to prevent olive beads migration and embedded into fracture fragments. The fragments were pulled first adequately with a tensioner to reduce the fragments before being locked and tensioned appropriately.
b. Alternative options - the key fragments reduced using K-wires as a joystick or mini-open if any disimpaction of fracture fragments needed

Figure 2: Olive wire inserted over the fracture fragments and intra-fragmentary compression achieved with tensioning on adjacent frames
In open injury, further wound management was done with regular dressing or vacuum dressing. Patients were taught to do regular pin site dressing. Depending on the severity of the injury, weight-bearing was permitted as soon as possible once tolerated by patients. In adjunct, physiotherapy commenced with the aim to regain range of motion of hip and knee joints, early weight-bearing as well as prevention of oedema and deep vein thrombosis. Holistic management with physiotherapists was of utmost importance to restore patients’ function almost immediately in terms of global joint range of motion and ambulation on the frame. This aided patients tremendously in terms of physical as well as psychological support. Patients were routinely followed up and assessment was done clinically and radiographically. The Ilizarov External Fixator has been removed as soon as 3 months post-operation. Functional outcome was assessed using the American Orthopaedic Foot and Ankle Society (AOFAS), Foot and Ankle Disability Index (FADI) score, and VAS - pain scales at 1-year post-trauma. [3,4,5] We reported four cases of patients with ankle injuries over the malleolar area and treated with Ilizarov External Fixator.
Case 1 (Figure 3)
A 39-year-old man presented with an open left bimalleolar fracture with syndesmotic joint disruption (Pronation-External Rotation III) with injury graded as Gustilo Type II. The patient was treated with initial wound debridement and spanning external fixator, but soft tissue condition did not allow for safe conversion to internal fixation even after 1-month post-trauma.

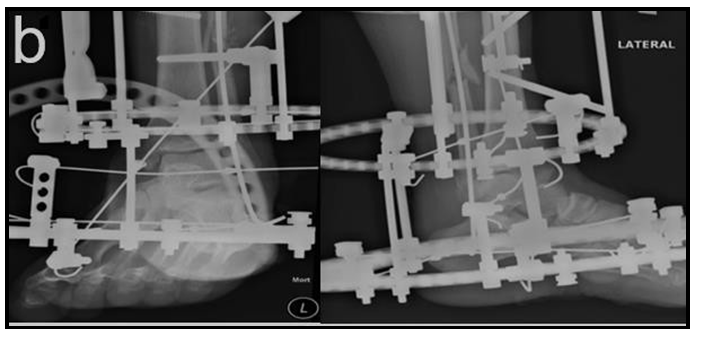

Figure 3: a) Open wound with skin abrasion of the left ankle, b) Ilizarov fixation to the fracture, c) Radiograph post Ilizarov fixation 4 keys technique used in this IEF fixation
Intramedullary wire over the fibula
Tensioned olive wire to reduce syndesmotic joint
Tensioned olive wire with washer as interfragmentary compression over the medial malleolus fracture
Tensioned olive wire from lateral to medial direction to reduce talar subluxation
Case 2 (Figure 4)
A 19-year-old man presented with open right trimalleolar fracture dislocation, Gustilo Type IIIa but complicated with ankle septic arthritis following motor vehicle accident. He underwent wound debridement and spanning external fixator and further revisited for multiple wound debridement and washout. He subsequently underwent Ilizarov External Fixator after about 1 month post trauma.

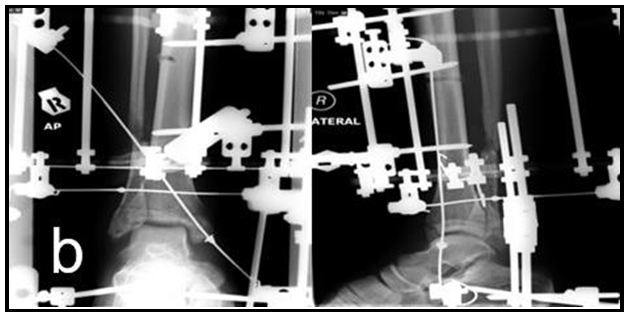
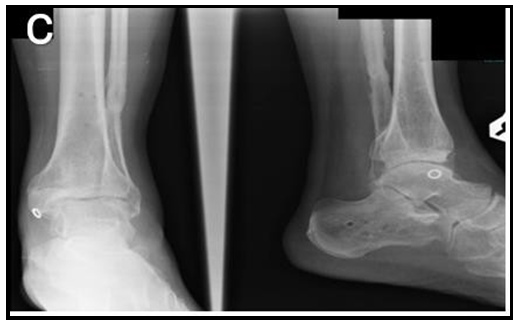
Figure 4: a) Infected wound after initial stabilisation right ankle, b) Ilizarov fixation to the fracture, c) Radiograph post Ilizarov fixation.
In this case, reduction done via percutaneous methods with 3 tensioned olives wires used to provide interfragmentary compression on medial malleolus, posterior malleolus and realignment of lateral malleolus fracture fragments.
Case 3 (Figure 5)
A 44-year-old man with closed right trimalleolar fracture following motor vehicle accident. Patient presented late with deformed ankle on poor temporary immobilisation from outpatient setting. Skin condition was extremely not suitable for internal fixation with Tscherne Classification Grade 2. Patient underwent Ilizarov External Fixator surgery. In this case, reduction was done via percutaneous methods with 2 tensioned olives wires used to provide interfragmentary compression on medial malleolus and posterior malleolus.


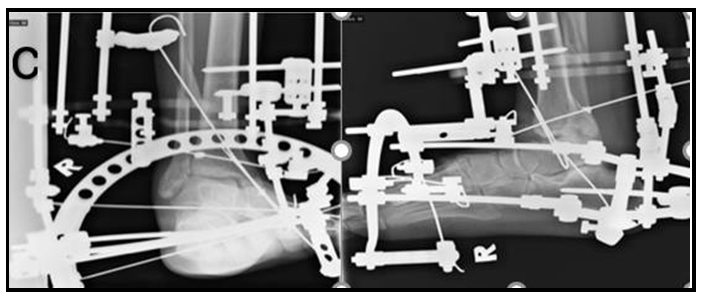
Figure 5: a} Radiograph showed right trimalleolar fracture, b) Ilizarov fixation to right lower limb, c) Radiograph post Ilizarov fixation
Case 4 (Figure 6)
A 45-year-old lady with history of motorvehicle accident, sustained open trimalleolar fracture left ankle with subtalar joint subluxation (Supination-External Rotation type IV), classified as Gustilo Type II.
She underwent Ilizarov External Fixator surgery with olive wires over medial malleolus and posterior malleolus as well as intramedullary rod of fibula.
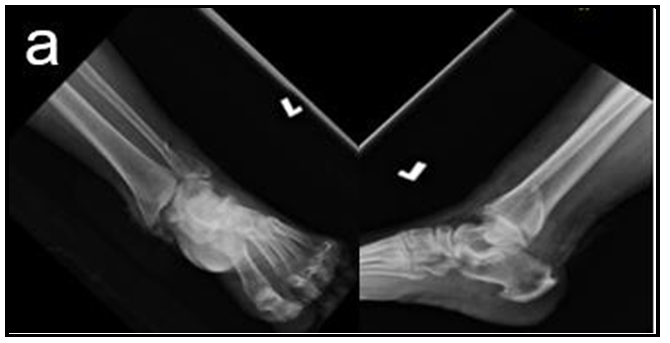
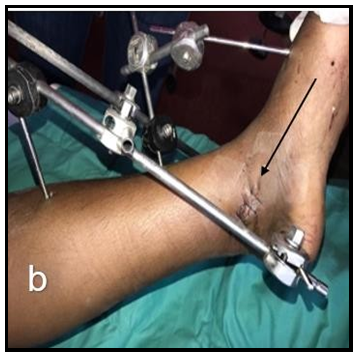
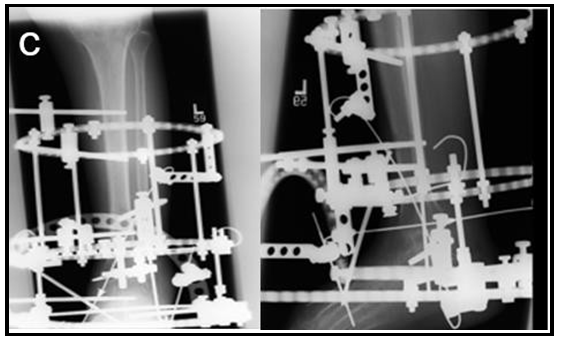
Figure 6: a) Radiograph of left trimalleolar fracture, b) Black arrow to show deep open wound which have been sutured, c) Radiograph of post Ilizarov fixation
All of the patients in this case series demonstrated mild and occasional pain but ambulating without any walking aid. Nevertheless, gait pattern was affected slightly with limitation on recreational activities.
The positive findings are good, plantigrade foot, ankle-hindfoot well aligned with stable ankle-hindfoot (anteroposterior, varus-valgus). Due to trans-fixation over calcaneal and spanning ankle fixation, all patients suffered from moderate restriction of sagittal motion (flexion plus extension) and hindfoot motion (inversion plus eversion).
The results are as followed:
|
Patient |
Age |
Fracture |
Time on Frame (weeks) |
AOFAS score |
FADI score |
VAS score |
|
Post IEF removal |
||||||
|
1 |
39 |
Open left bimalleolar fracture with syndesmotic joint disruption |
14 |
85 |
83 |
1 |
|
2 |
19 |
Open right trimalleolar fracture-dislocation |
14 |
80 |
80 |
2 |
|
3 |
44 |
Closed right trimalleolar fracture |
12 |
82 |
79 |
1 |
|
4 |
45 |
Open trimalleolar fracture left ankle with subtalar joint subluxation |
16 |
78 |
81 |
2 |
|
Average |
14 |
81.3 |
80.8 |
1.5 |
||
In all patients, none ended up with persistent soft tissue and bone infection during course of treatment and following subsequent frame removal.
Discussion
Fractures around the ankle, in particular malleoli fracture may cause extensive damage to both soft tissues and bones. The advent of minimally invasive technique of internal fixation with supplementation of other methods of fixation such as tightrope shows that much effort has been made to fix this precarious area. Nevertheless, the daunting aspect of postoperative infections with subsequent operations may hinder this recent concept of fixation. Sherif et. al showed that almost none of their patients developed soft tissue infection in minimally invasive surgery but only 36 % patients experienced an excellent outcome.[6] In contrast, 23 patients (55 %) had a good, 3 (7 %) a fair, and 1 (2.5 %) a poor outcome. Meredith et al. on the other hand showed that about 1.5 % of her series developed early postoperative infection in particular group of high-risk patients such as slightly older on average, diabetes, and had higher anaesthesia class.[7] Tarchokov et al. in his series of ankle fracture fixation with Ilizarov External Fixator showed no infection with good outcome.[8] In our case series, reduction of intraarticular fragments and ankle mortise position were achieved via indirect reduction with Image Intensifier guidance. In our opinion, despite non anatomic reduction achieved unlike open reduction, we were able to provide stable anatomic reduction of talus in the ankle mortise in all cases. This technique is very important as 1 mm shift of talus may lead to 42 % decrease in tibiotalar contact area. [9] Long term complication of this fracture may lead to post traumatic arthrosis as high as 60-70 % as reported by Anne Lubbeke et al. in their long term follow up study.[10] Besides, temporary distraction allows fracture healing to take place and union occur before possibility of any fracture fragments redisplacement or collapse and thus ultimately lead to failure. This aim is in line with postulation of Buckwalter et al. that distraction reduces mechanical stress joint, protect the remaining cartilage, and even allow for cartilage reparation.[11]
In all of our patients, the Ilizarov External Fixator fixation was fixed across the ankle until frame removal. This lead to joint stiffness but all of our patients showed satisfactory functional results on walking plus stability of the ankle. This may confer them to walk and resume normal daily activities but participation in highly functional ankle demand activities might be severely affected. Despite this, in long term study of open reduction internal fixation of S. M. Verhage et al. on 243 patients with malleolar fractures, he noted similar restriction on dorsiflexion of 2.9° vs 6.9° occurred in unimalleolar fracture and worse in trimalleolar fractures.[12]
Despite promising results, the drawbacks of the Ilizarov External Fixator technique are the risk of losing full range of movement of the ankle joint and the visually less appealing and cumbersome ring external fixator. In addition, it is also a very demanding technique with a steep learning curve, requiring specialised training and experience.
Conclusion
We believe that fracture fixation over malleoli area in a non-desirable soft tissue condition with Ilizarov External Fixator will yield a satisfactory and good outcome. It reduces almost to non-possible surgical site infection with advantages of early weight bearing and non-implant retention.
References
- Tscherne H, Oestern HJ (1982) [A new classification of soft- tissue damage in open and closed fractures (author’s transl)] [in German] Unfallheilkunde. 85(3): 111–115.
- Gustilo RB, Anderson JT (1976) Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 58(4): 453–458.
- Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, et al. (1994) Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int.; 15(7): 349–53.
- Martin RL, Burdett RG, Irrgang JJ, Martin, Martin RL,et al. (1999) Development of the foot and ankle disability index (FADI). J Orthop Sports Phys Ther 29. 1: A32-A33.
- McCormack HM, Horne DJ, Sheather S (1988) Clinical applications of visual analogue scales: a critical review. Psychol Med 18(4): 1007-1019.
- Abdelgaid SM, Moursy AF, Allah Elgebaly EA, Aboelenien AM (2018) Minimally Invasive Treatment of Ankle Fractures in Patients at High Risk of Soft Tissue Wound Healing Complications. J Foot Ankle Surg. 57(3): 557-571.
- Schade MA, Hollenbeak CS (2018) Early Postoperative Infection Following Open Reduction Internal Fixation Repair of Closed Malleolar Fractures. Foot Ankle Spec. 11(4): 335-341.
- Tarchokov VT, Leonchuk SS (2017) Ilizarov Technique in Acute Ankle Trauma: A Report of Fourth Cases. Emerg Med (Los Angel). 7(2): 352.
- Ramsey PL, Hamilton W (1976) Changes in tibiotalar area of contact caused by lateral talar shift. Bone Joint Surg Am. 58(3): 356-7.
- Lübbeke A, Salvo D, Stern R, Hoffmeyer P, Holzer N, et al. (2012) Risk factors for post-traumatic osteoarthritis of the ankle: an eighteen-year follow-up study. Int Orthop. 36(7): 1403-10.
- Buckwalter JA, Mankin HJ (1998) Articular cartilage: degeneration and osteoarthritis, repair, regeneration, and transplantation. Instr Course Lect. 47: 487–504
- Verhage SM, Schipper IB, Hoogendoorn JM (2015) Long-term functional and radiographic outcomes in 243 operated ankle fractures. J Foot Ankle Res. 8: 45.