


Yusuf Omar Qalib*#, Sunil Dachepalli*#, Srinivasa Reddy Medagam, Lokesh Kumar Gupta
Department of Orthopaedics, Yashoda Hospitals, Somajiguda, Hyderabad, Telangana, India, 500082
#Dr. Yusuf Omar Qalib and Dr. Sunil Dachepalli contributed equally to this work.
*Corresponding Author: Yusuf Omar Qalib & Sunil Dachepalli, Pharmacovigilance Programme of India, National Coordination Centre, Indian Pharmacopoeia Commission, Ghaziabad, India.
Abstract
Purpose: In the setting of anterior cruciate ligament (ACL) rupture, the repair is still avoided by some surgeons in favour of reconstruction. The latter has been considered a gold standard approach for many decades due to poor postoperative outcomes following ACL repair. However, the main advantage of ACL repair, which is the preservation of the native ligament, cannot be ignored.
Methods: Patients with partial ACL tear that underwent ACL tightening from 2019 to 2022 were included. Baseline characteristics (gender, age, BMI, injury mechanism, time from injury to surgery, concomitant injuries, preoperative and postoperative anterior drawer test, Lachman test, and Modified cincinnati knee rating system) were collected.
Results: A total of 14 patients (mean age: 32.1±6.3 years, range: 19-42 years) diagnosed with a partial ACL tear on MRI underwent a modified suture tape augmentation. The mean follow-up was 31.1±7.7 months (range: 24-44 months). During the follow-up, no major complications were observed, and none of the patients required ACLR. Treatment was successful in 100% of patients. Postoperative Lachman and anterior drawer tests were negative, the mean modified cincinnati rating system scores 3 months, 6 months, 12 months, and 24 months after surgery were 79.1±9.4, 92.4±5.4, 96.3±2.3, and 98.9±1.7, respectively.
Conclusion: This technique is not only safe but also straightforward and competent, as it results in excellent patient outcomes.
Keywords: anterior cruciate ligament, ACL repair, suture tape augmentation, case series
Abbreviations: ACL: anterior cruciate ligament, ACLR: anterior cruciate ligament reconstruction, BMI: body mass index, RTA: road traffic accident, MM: medial meniscus, LM: lateral meniscus, MCL: medial collateral ligament, MCRS: Modified Cincinnati Rating System.
Introduction
ACL repair is still neglected by many surgeons due to very poor postoperative outcomes reported in the past [1,2]. Orthopedics usually opt out of performing ACL repair even when feasible (e.g., sufficient remaining ACL tissue), inclining towards more “orthodox” ACL reconstruction (ACLR). However, ACL repair is gaining more and more attention after a growing number of publications showing satisfactory short-term and mid-term postoperative outcomes [3]. Contrary to common belief, ACL can heal and was shown to heal even in complete ruptures[4,5]. This healing potential possessed by ACL, combined with the fact that some patients receiving ACLR present with a significant portion of intact ACL tissue, indicates that the management of ACL rupture requires careful consideration and weighing each treatment method rather than immediately selecting ACLR. There are four main techniques used for ACL repair: dynamic intraligamentary stabilization, suture tape augmentation, also known as internal brace ligament augmentation, suture anchor primary repair, and bridge-enhanced repair. All of them have their applications, advantages, and disadvantages[6-9]. This article describes 14 cases of partial ACL tears that were treated with ACL tightening and had at least two years of follow-up.
Materials and Methods
Patients with a partial ACL tear that underwent ACL tightening performed by the same surgeon in our institution from 2019 to 2022 were included. Exclusion criteria were as follows: follow-up <24 months, >grade II tear, remnant ACL tissue of poor quality, insufficient remnant ACL tissue length, revision surgeries, and increased laxity in the hyperflexed knee (Figure 1). Continuous variables were presented as mean ± standard deviation (SD), and categorical variables were presented as percentages. Informed consents were obtained from all the patients, and the study was approved by an ethics committee of our hospital.
Surgical technique
The detailed characteristics of patients are provided in Table 1. All patients were positioned supine with lateral post support to the mid- thigh and were given combined spinal and epidural anaesthesia. Following the creation of standard portals (anterolateral and anteromedial portals), the ACL was probed and found to be lax. Before deciding on ACL tightening, an arthroscopic evaluation was carried out to assess the intact ACL. Only then the decision to perform the ACL tightening was made. After the knee was positioned in hyperflexion, a femoral footprint tunnel was created through the anteromedial working portal using a 4.5 mm guide pin. With the drill guide still in place, the No. 2 Ethibond loop was passed through the guide pin, and the suture was placed approximately between the middle and proximal portions of the ACL. The ACL was then reinforced with Fiber Tape. The augmentation suture was loaded back into the self-retrieving suture passing device (Suture Lasso or FIRSTPASS Suture Passer), and the procedure was repeated 3-4 times until the ACL was sufficiently tightened (Figure 2,3). Under arthroscopic visualization, the free ends of Fiber Tape were pulled through the femoral tunnel using the No. 2 Ethibond loop. A small incision was made on the lateral aspect of the lateral epicondyle, and the exit site of the Fiber Tape was identified. Then, both edges of Fiber Tape were passed through Endo Button and tightened over the lateral epicondyle using a knot pusher (Figure 4). A suture cutter was used to remove the excess suture material. Next, the ACL was probed, the tightness was confirmed under arthroscopy, and the incision was closed. Finally, after the ACL tightening, all patients were evaluated again, including the anterior drawer test, Lachman test, and modified cincinnati knee rating system.
Postoperative rehabilitation included six weeks of knee range of motion of 0-90 degrees while using a full weight-bearing walker.
This study includes observations of 14 patients for which statistical analysis such as pre and post operative mean and standard deviation were calculated.
Table 1: Patient characteristics
|
No. |
Sex |
Age (years) |
BMI |
Follow-up (months) |
Injury mechanism |
Time from injury to surgery (months) |
Concomitant injuries |
Anterior drawer test |
Lachman test |
|
|
MCRS |
|
|
||
|
|
|
|
|
|
|
|
Preop |
Postop |
Preop |
Postop |
Preop |
3 months postop |
6 months postop |
12 months postop |
24 months postop |
|
|
1 |
M |
32 |
25.2 |
44 |
Fall |
2 |
MM injury |
+ |
- |
+ |
- |
64 |
60 |
76 |
94 |
100 |
|
2 |
F |
34 |
25.8 |
41 |
Fall |
31 |
None |
+ |
- |
+ |
- |
48 |
84 |
96 |
98 |
98 |
|
3 |
F |
33 |
19.6 |
41 |
Sports (tennis) |
3 |
MM injury |
+ |
- |
+ |
- |
77 |
70 |
92 |
96 |
96 |
|
4 |
M |
29 |
26.7 |
40 |
Fall |
14 |
MM injury |
+ |
- |
+ |
- |
54 |
80 |
90 |
100 |
100 |
|
5 |
M |
24 |
30.5 |
36 |
Fall |
1 |
None |
+ |
- |
+ |
- |
34 |
94 |
96 |
100 |
100 |
|
6 |
M |
32 |
26.9 |
32 |
RTA |
7 |
None |
+ |
- |
+ |
- |
40 |
90 |
94 |
94 |
100 |
|
7 |
M |
19 |
23.9 |
28 |
Sports (cycling) |
6 |
None |
+ |
- |
+ |
- |
36 |
78 |
92 |
94 |
100 |
|
8 |
M |
39 |
25.2 |
26 |
Sports (exercising) |
2.5 |
None |
+ |
- |
+ |
- |
44 |
81 |
96 |
96 |
100 |
|
9 |
M |
27 |
25 |
25 |
Sports (running) |
4 |
None |
+ |
- |
+ |
- |
42 |
74 |
90 |
94 |
100 |
|
10 |
M |
40 |
26.3 |
25 |
Sports (football) |
5 |
None |
+ |
- |
+ |
- |
60 |
76 |
96 |
96 |
100 |
|
11 |
M |
29 |
25.5 |
25 |
Sports |
12 |
MM and LM injuries |
+ |
- |
+ |
- |
30 |
90 |
98 |
100 |
100 |
|
12 |
F |
34 |
21.6 |
24 |
Fall |
21 |
MM, LM and MCL injuries |
+ |
- |
+ |
- |
32 |
66 |
90 |
96 |
100 |
|
13 |
M |
36 |
30.1 |
24 |
Fall |
12 |
MM and LM injuries |
+ |
- |
+ |
- |
40 |
82 |
94 |
94 |
96 |
|
14 |
M |
42 |
28.4 |
24 |
Sports (running) |
2 |
MM injury |
+ |
- |
+ |
- |
54 |
82 |
94 |
96 |
96 |
Note: RTA – road traffic accident, MM – medial meniscus, LM – lateral meniscus, MCL – medial collateral ligament, MCRS– Modified Cincinnati Rating System. Range for MCRS score is 0to 100.
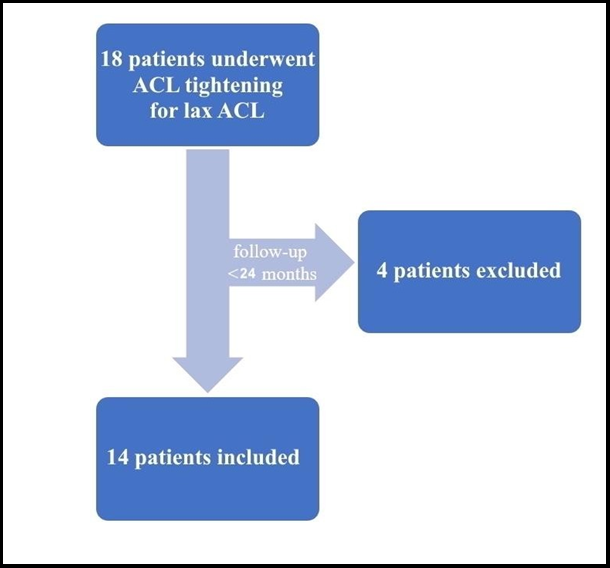
Figure 1: Flowchart of inclusion criteria.
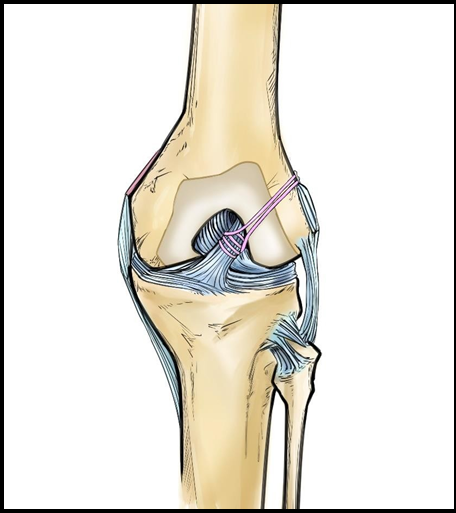
Figure 2: Illustration of anterior cruciate ligament tightening.
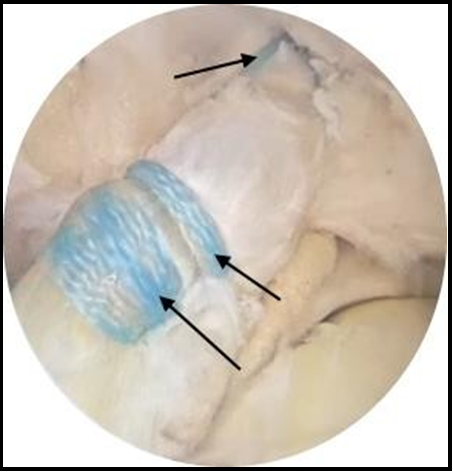
Figure 3: Repaired anterior cruciate ligament using suture tape augmentation (arrow).
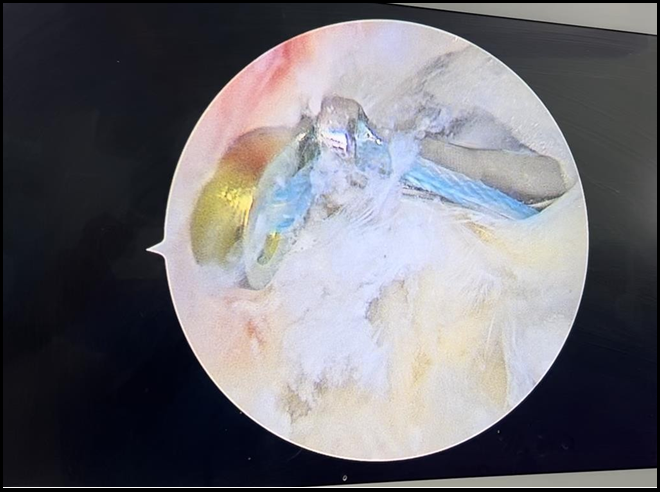
Figure 4: Endo Button placement and knot pusher.
Results
A total of 18 patients diagnosed with a partial ACL tear on MRI underwent ACL tightening (Figure 5). Four patients were lost to follow-up and thus excluded. So, 14 patients were included in the final study. Among them, there were 11 males (78.6%) and 3 females (21.4%). The mean age was 32.1±6.3 years (range: 19-42 years). 11 patients (78.6%) presented as overweight, and the mean BMI was 25.8±2.9. Seven patients (50.0%) obtained their injury during playing sports (one patient had unspecified sports injury), whereas ACL tear due to fall and traffic accident was observed in six (42.9%) and one (7.1%) patient, respectively. The mean time from onset to injury was 8.75±8.6 months. Half of the patients did not have any concomitant injuries, and medial meniscus injury alone or combined with other injuries was present in the rest. All the patients had positive anterior drawer test and Lachman test, whereas the mean preoperative Modified cincinnati knee rating system was 46.8±13.6.
After surgery, all the patients reported their condition as satisfactory. The mean follow-up was 31.1±7.7 months (range: 24-44 months). During the follow-up, no major complications were observed, and none of the patients required ACLR. Postoperative Lachman and anterior drawer tests were negative, the mean Modified cincinnati knee rating system 3 months, 6 months, 12 months, and 24 months after surgery was 79.1±9.4, 92.4±5.4, 96.3±2.3, and 98.9±1.7, respectively.
Discussion
Our technique is a modification of the suture tape augmentation technique that results in even better knee healing, increases knee stability, and improves patient outcomes (Table 2). All the included patients were diagnosed with partial ACL tears, and the vast majority of them had grade II tear, whereas grade I was present only in a handful of the included patients. The decision to perform ACL tightening was made intraoperatively after careful probing, or to be more precise, after evaluating the state of the native ACL. As such, patients with a partial ACL tear but with insufficient remnant ligament tissue could not go undergo ACL tightening. Such meticulous patient selection showed excellent results: despite concomitant injuries, none of the 14 patients required ACLR during the follow-up. Patient selection is one of the most crucial steps in this procedure, as ACL repair has unclear long-term outcomes and several disadvantages that must be taken into account [10]. It is especially important in younger patients. For instance, despite strict criteria for treatment, pediatric patients (13.9±3.2 years old) with an ACL tear that received suture ligament augmentation repair showed very poor results with graft failure rate reaching as high as 48% within 3 years [11]. Nevertheless, one of the biggest advantages of ACL repair is that the native ACL is preserved. Apart from that, it does not have the same pitfalls that ACLR suffers from, such as a low rate of return to sports, excessive muscular atrophy, etc. [12,13]
A few studies on the modification of suture tape augmentation were published [14-16]. In this technique, we used Endo Button instead of an anchor. In our opinion, this increases the strength of the repair and decreases damage to the adjacent structures. Also, Endo Button is less expensive, and, in case of repair failure, ACLR would be easier to perform. However, both anchor and Endo Button have a major potential disadvantage in the form of postoperative displacement [17]. A new study reported that ACL repair (suture anchor) was associated with greater meniscal preservation compared to ACLR [18]. In our study, seven patients had concomitant medial meniscus injury, but we did not assess the rate of repair of medial meniscus in them, and this was beyond the scope of the present study.
According to a recent cadaveric study, in a femoral avulsion model, valgus, varus, internal, or external rotation of knees that underwent ACL augmentation repair (internal brace) are similar to those that underwent ACLR, and anterior tibial translation was restored in both groups [19]. In addition, ACL suture augmentation repair has a low failure rate and results in improvement of functional knee scores in the short-term. However, adolescent failure rates were higher than in adult rates [20]. Another meta-analysis reported similar outcomes between ACL repair and ACLR. Interestingly, functional performance was higher in the patients that underwent ACL repair, but at the same time they had more frequent hardware removal and asymptomatic knee laxity[21]. Overall, suture tape augmentation has demonstrated satisfactory results in selected patients both in the short- and long-term [22-24]. However, the reported failure rate is far from perfect. In this study, all the patients had an improvement in all physical tests and modified cincinnati knee rating system. Moreover, there was no single patient that developed a repair failure during the follow-up. Unfortunately, no specific rehabilitation protocols exist for ACL repair, so they are largely based on the surgeon’s experience [25]. We selected postoperative rehabilitation protocol on the basis of stress reduction applied to the knee and quicker recovery without any significant complications.
Conclusion
This technique results in excellent outcomes following careful intraoperative patient selection. All the patients had an improvement in postoperative Anterior drawer test, Latchman test, and modified cincinnati knee rating system (3,6,12 and 24 months after surgery), and none of the patients developed repair failure. This procedure is not only safe but also straightforward and competent.
Pearls
1. Tightening of the ACL without creating microfractures or using anchor.
2. EndoButton is used for fixation.
3. Increased repair strength and decreased structural damage.
Pitfalls
1. Careful patient selection: good quality and sufficiently long remnant ACL tissue is required.
2. EndoButton may potentially migrate.
Limitations
Our study has several limitations. Firstly, due to the small sample size, we only included 14 cases with a partial ACL tear that underwent ACL tightening and had at least a 24-month follow-up. Secondly, no comparative study has been conducted to compare the outcomes of ACL augmentation and ACLR. We do not, however, have any follow- up MR images or second view arthroscopy to assess the progress of healing at the augmentation site. A follow-up of more than 24-months is needed.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Funding: None
Ethical approval
This study was approved by the local ethics committee. Informed consent was obtained from the patients.
Acknowledgement: None
Author’s contributions
D.S had full access to all of the data in the study and take responsibility for the data’s integrity and the accuracy. Concept and design: Q.Y.O, D.S. Acquisition, analysis, or interpretation of data: Q.Y.O, M.S.R. Drafting of the manuscript: Q.Y.O, G.L.K, Critical review of the manuscript for important intellectual content and editing: All authors.
References
- Uchida R, Jacob G, Shimomura K, Horibe S, Nakamura N (2020) Biological Augmentation of ACL Repair and Reconstruction: Current Status and Future Perspective. Sports Med Arthrosc Rev. 28(2): 49-55.
- Taylor SA, Khair MM, Roberts TR, DiFelice GS (2015) Primary Repair of the Anterior Cruciate Ligament: A Systematic Review. Arthroscopy. 31(11): 2233-2247.
- Smith PA (2021) Editorial Commentary: Repair the Anterior Cruciate Ligament When You Can: Add Suture Tape Augmentation and Dress for Success. Arthroscopy. 37(4): 1242- 1244.
- Muller B, Bowman KF Jr, Bedi A (2013) ACL graft healing and biologics. Clin Sports Med. 32(1): 93-109.
- Costa-Paz M, Ayerza MA, Tanoira I, Astoul J, Muscolo DL (2012) Spontaneous healing in complete ACL ruptures: a clinical and MRI study. Clin Orthop Relat Res. 470(4): 979-985.
- Heusdens CHW (2021) ACL Repair: A Game Changer or Will History Repeat Itself? A Critical Appraisal. J Clin Med. 10(5): 912.
- Perera J, Miller MD, Danahy P (2022) Case Report Demonstrating Multifactorial Risks of Anterior Cruciate Ligament Re-tear Injuries and Appropriate Response Among Those With High Chance of Recurrence. Cureus. 14(5): e24965.
- Cristiani R, Mouton C, Siboni R, Pioger C, Seil R (2022) Failure of primary ACL repair with dynamic intraligamentary stabilization may result in a high risk of two-stage ACL reconstruction: a case series of ten patients. J Exp Orthop. 9(1): 79.
- Weninger P, Wepner F, Kissler F, Enenkel M, Wurnig C (2015) Anatomic Double-Bundle Reinsertion After Acute Proximal Anterior Cruciate Ligament Injury Using Knotless PushLock Anchors. Arthrosc Tech. 4(1): e1-e6.
- Batista JP, Chahla J, Dalmau-Pastor M, Maestu R, Kunze KN, et al. (2021) Arthroscopic anterior cruciate ligament repair with and without suture augmentation: technical note. J ISAKOS. 6(4): 251-256.
- Gagliardi AG, Carry PM, Parikh HB, Traver JL, Howell DR, et al. (2019) ACL Repair With Suture Ligament Augmentation Is Associated With a High Failure Rate Among Adolescent Patients. Am J Sports Med. 47(3): 560-566.
- Samuelsen BT, Webster KE, Johnson NR, Hewett TE, Krych AJ (2017) Hamstring Autograft versus Patellar Tendon Autograft for ACL Reconstruction: Is There a Difference in Graft Failure Rate? A Meta-analysis of 47,613 Patients. Clin Orthop Relat Res. 475(10): 2459-2468.
- Sepúlveda F, Sánchez L, Amy E, Micheo W (2017) Anterior Cruciate Ligament Injury: Return to Play, Function and Long- Term Considerations. Curr Sports Med Rep. 16(3): 172-178.
- Youssefzadeh KA, Stein SM, Limpisvasti O (2020) Anterior Cruciate Ligament Repair Using a Knotless Suture Implant. Arthrosc Tech. 9(5): e623-e626.
- Achtnich A, Herbst E, Forkel P, Metzlaff S, Sprenker F, et al. (2016) Acute Proximal Anterior Cruciate Ligament Tears: Outcomes After Arthroscopic Suture Anchor Repair Versus Anatomic Single-Bundle Reconstruction. Arthroscopy. 32(12): 2562-2569.
- Zhao L, Lu M, Deng M, Xing J, Xu T (2020) Arthroscopy Primary Double-Bundle Repair of Anterior Cruciate Ligament With Internal Brace Augmentation and a Knotless Anchor Implant. Arthrosc Tech. 9(12): e1927-e1935.
- Jin C, Paluvadi SV, Lee S, Yoo S, Song EK, et al. (2018) Biomechanical comparisons of current suspensory fixation devices for anterior cruciate ligament reconstruction. Int Orthop. 42(6): 1291-1296.
- Wilson WT, Hopper GP, Hamilton C, O'Donnell L, Blyth MJG, et al. (2022) Meniscal Preservation is More Likely When Performed with Acute Anterior Cruciate Ligament Repair Rather Than with Anterior Cruciate Ligament Reconstruction. Surg Technol Int. 40: 341-345.
- Chahla J, Nelson T, Dallo I, Yalamanchili D, Eberlein S, et al. (2020) Anterior cruciate ligament repair versus reconstruction: A kinematic analysis. Knee. 27(2): 334-340.
- Vermeijden HD, van der List JP, Benner JL, Rademakers MV, Kerkhoffs GMMJ, et al. (2022) Primary repair with suture augmentation for proximal anterior cruciate ligament tears: A systematic review with meta-analysis. Knee. 38: 19-29.
- Pang L, Li P, Li T, Li Y, Zhu J, et al. (2022) Arthroscopic Anterior Cruciate Ligament Repair Versus Autograft Anterior Cruciate Ligament Reconstruction: A Meta-Analysis of Comparative Studies. Front Surg. 9: 887522.
- Hopper GP, Aithie JMS, Jenkins JM, Wilson WT, Mackay GM (2022) Satisfactory patient-reported outcomes at 5 years following primary repair with suture tape augmentation for proximal anterior cruciate ligament tears. Knee Surg Sports Traumatol Arthrosc. 30(1): 253-259.
- Heusdens CHW, Blockhuys K, Roelant E, Dossche L, Van Glabbeek F, et al. (2021) Suture tape augmentation ACL repair, stable knee, and favorable PROMs, but a re-rupture rate of 11% within 2 years. Knee Surg Sports Traumatol Arthrosc. 29(11): 3706-3714.
- Steadman JR, Matheny LM, Briggs KK, Rodkey WG, Carreira DS (2012) Outcomes following healing response in older, active patients: a primary anterior cruciate ligament repair technique. J Knee Surg. 25(3): 255-260.
- Wu J, Kator JL, Zarro M, Leong NL (2022) Rehabilitation Principles to Consider for Anterior Cruciate Ligament Repair. Sports Health. 14(3): 424-432.