


Brian Hynes MD FRCS© FACS1, Brian Blakley MD Ph.D. FRCS©2, Amanda Alcaide3*
1Blue Water Health Sarnia, Adjunct Professor Otolaryngology University of Western Ontario, London Ontario, Canada
2Professor Department of Otolaryngology, University of Manitoba, Winnipeg Manitoba, Canada.
3Second-year Neuroscience B.Sc. (Hons) student, University of Western Ontario, London Ontario, Canada
*Corresponding Author: Amanda Alcaide, second-year Neuroscience B.Sc. (Hons) student, University of Western Ontario, London Ontario, Canada.
Abstract
Idiopathic unilateral sudden sensorineural hearing loss is not uncommonly seen in clinical practice. Although a specific etiology is not usually identified, steroids are often prescribed with the hope of some return of function. The authors present an unusual case of hearing return many years after the onset of hearing loss.
Keywords: Sudden neural hearing loss, Otolaryngology, ENT, case report
Case Description
A 26-year-old nursing student presented for an audiogram (Figure 1: Audiogram Legend). Seen nine years earlier by the senior author, she had recently become aware of an increase in her hearing acuity. She presented as a teen with a sudden left SNHL and tinnitus without dizziness. There had been no history of illness or otic trauma, and she was initially treated at the emergency room (ER) with a course of prednisone. An ENT consult was arranged. Her past medical historywas non-contributory, and the ENT exam was within normal. Her initial audiogram showed normal right-sided hearing and a left moderate to severe SNHL with an SRT of 55dB and a WDS of 72 % (See Figure 2). An IAC MRI was done and was normal. A second course of oral prednisone was prescribed, but follow-up audiograms showed no improvement (See Figure 3 and 4).
Figure 1: Audiogram Legend
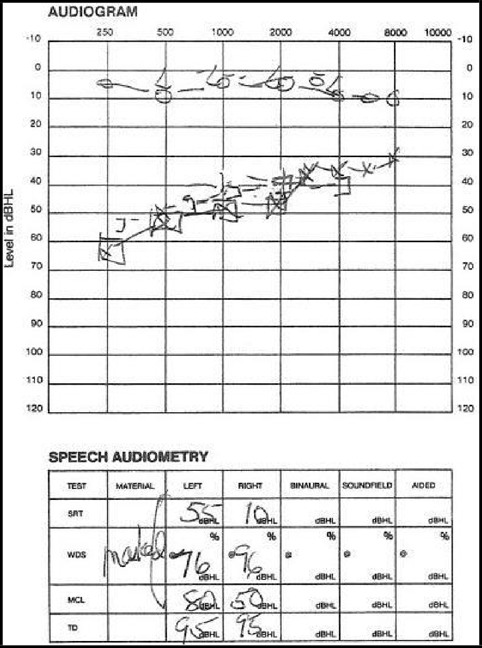
Figure 2: First Audiogram of Patient December 17, 2008
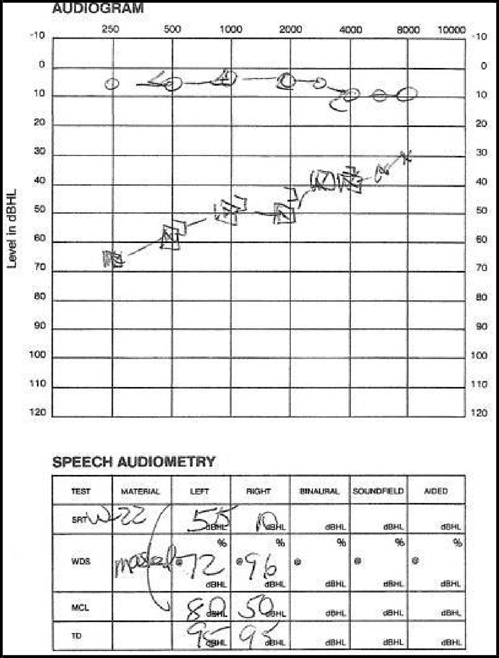
Figure 3: Second Audiogram January 6, 2009
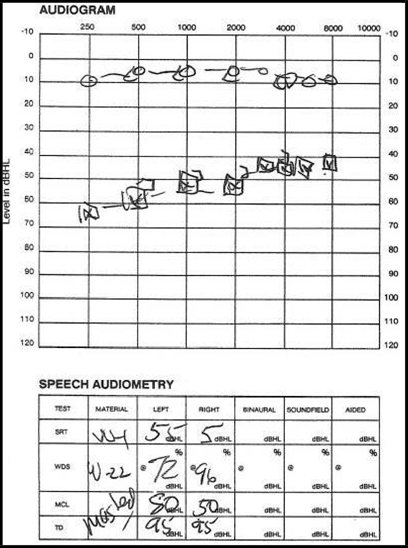
Figure 4: Third Audiogram January 20, 2009
Her diagnosis at that time was idiopathic, left sudden SNHL, which did not respond to the steroid therapy. The patient and her family were told that it was possible that her hearing would not return. However, follow-up audiograms were recommended, but the patient was not seen again for follow-up.
When seen for an audiogram at her request, the patient explained that while recently studying for finals as a nursing student, she began to experience and was diagnosed with left-sided migraine headaches, which were consistently associated with a throbbing left pulsation. After each migraine episode, the patient noticed a slight improvement in her left hearing acuity and a decrease in her left tinnitus. As a result, she felt a new audiogram was in order, and when done by the same otolaryngologist using the same audiometer and performed by the same audiologist almost ten years later, her hearing was normal. She had, as she perceived, bilateral normal hearing levels with WDS of 100% and SRT levels of 5dB (See Figure 5).

Figure 5: Fourth Audiogram May 15, 2018
Discussion
By definition, the primary cause of idiopathic sudden sensorineural hearing loss is unknown. The two most likely causes are 1) immune activation, perhaps initiated by a virus, and 2) obstruction of the artery of the internal auditory canal (IAC). Clinically it is difficult to distinguish between the two. There is no effective treatment for obstruction of the artery of the IAC, but immune dysfunction could be mitigated by corticosteroid administration, so treatment has focused on systemic and intratympanic steroid administration. Perhaps 59 % of SSHL patients treated within 10 days experienced “recovery” to some extend [1], but variability in definitions, specific treatments, and evaluation make comparisons across the literature difficult to generalize.
Spontaneous recovery rates without treatment have been estimated at 50% [2]. “Improvement rates” of 59% [1], 66-85% [3], and similar rates have been reported with better results if treatment is initiated early[1,4]. Numerous publications have identified the weakness in the research on this topic.
Despite the controversy, the current consensus is that SNHL, which does not improve after 2-4 weeks, is unlikely to improve even with treatment. It is recommended that treatment begins by that time [5]. Initial treatment with systemic corticosteroids with salvage intratympanic steroid injection has been suggested in a guideline of the American Academy of Otolaryngology-Head and Neck Surgery [5]. For the purposes of this report it would appear that spontaneous improvement of hearing years after the onset of SSHL is highly unlikely.
The subjective awareness of hearing improvement and a decrease in tinnitus cannot be objectively explained, but her clinical awareness of improved auditory function is correlated with her recent audiogram (see figure 5). Migraine attacks are complex neural events. Migraine sufferers, however, describe a pounding vascular headache with attacks that imply a degree of vasodilation at some point during the attack. The authors cannot explain the patient’s subjective sense of clinical improvement following each migraine attack but can validate her clinical history with audiometric testing, which showed improvement unexpectantly so many years after the onset of her hearing loss.
Conclusion
The authors present an interesting case of a patient with idiopathic sudden SNHL from nine years prior who experienced a remarkable improvement in her hearing acuity after repetitive migraine attacks over a short period of time. Although a specific etiology for such hearing loss is usually not detected, and there is not a particular universal treatment for this clinical entity, she did receive the often-prescribed courses of prednisone without effect.
Conflicts of Interests
None of the authors have any personal or financial conflicts of interest to report.
All authors had a significant contribution in writing and formatting the final version of the manuscript.
References
- Edizer DT, Çelebi Ö, Hamit B, Baki A, Yiğit Ö (2015) Recovery of Idiopathic Sudden Sensorineural Hearing Loss. J Int Adv Otol. 11(2): 122-126.
- Stew BT, Fishpool SJ, Williams H (2012) Sudden sensorineural hearing loss. Br J Hosp Med (Lond). 73(2): 86-89.
- Labatut T, Daza MJ, Alonso A (2013) Intratympanic steroids as primary initial treatment of idiopathic sudden sensorineural hearing loss. The Hospital Universitario Ramon y Cajal experience and review of the literature. Eur Arch Otorhinolaryngol. 270(11): 2823-2832.
- Metrailer AM, Babu SC (2016) Management of sudden sensorineural hearing loss. Curr Opin Otolaryngol Head Neck Surg. 24(5): 403-406.
- Chandrasekhar SS, Tsai Do BS, Schwartz SR, Bontempo LJ, Faucett EA, et al. (2019) Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol Head Neck Surg. 161(1_suppl): S1-S45.