


Abderrahmane Housni*, Zakariaa Chandide Telmçani, Imadeddine Sahri, Mamoune El Mostarchid, Sofia Elakroud, Freshnel Obam, Hugues Christian, El Kacemi Inas, Mohcine Salami, Brahim El mostarchide, Miloudi Gazaz
Military Hospital Mohamed V of Rabat, Morocco.
*Corresponding Author: Abderrahmane Housni, Military Hospital Mohamed V of Rabat , Morocco.
Abstract
Iatrogenic subdural empyema after spinal anesthesia is an extremely rare but serious complication with serious morbidity and mortality, The most causal agent according to littérature is the streptococcus, so we report here a case of a postpartum woman with a subdural empyema probably due to spinal anesthesia, she underwent an evacuation with antioibiotherapy, Radiological and biological exploration was important for the management of the patient.
Keywords: subdural empyema, epidural anesthesia, MRI, ct scan, bacteriology
Introduction
cesarean and Epidural anesthesia is a common practice in daily medical practice, however intrathecal administration of contaminated substances due to contaminated instruments or lack of asepsis in the puncture site can lead to serious complications as subdural empyema, including most of the time the Streptococcus pyogenes.
Case Presentation
We report here the case of a 23 years old woman with a history of a cesarean 15 days before admission performed in front of a stained amniotic fluid, in a peripheric center, which received epidural anesthesia during the operation, We couldn’t have information about spinal anesthesia conditions.
Initially, The patient was admitted to the emergency department for a brutal headache a fever with a little alteration of sensorium 13 days after the operation.
At first, a ct scan with an eye fundus was performed, then a lumbar puncture, the results were normal, also in order to understand the origin of the infection multiple biological exams were performed but there was no growth in blood, wound, or urine culture.
The blood test of the patient find no abnormalities except a leucocytosis 18000ul with 85 % neutrophils and RCP about 222 mg/l, Procalcitonin 0.07 her Coagulation profile was normal Since the clinical evolution worsens 48 hours later with the persistence of fever, and headache, a brutal alteration of consciousness with a gcs around 10-11 motivated ct scan of control it shows an important temporoparietal subdural collection suggestive of an empyema associated with cerebral edema, and a subarachnoid hemmoraghe .in front of this worst evolution our team decides to perform an evacuation of the collection by a parietal temporal craniotomy, the purulent material was sent to a laboratory, and a duraplasty was performed, the patient was admitted to the IUC for further management.
Finally, Micro bacterial analysis concludes with an enterobacter associated with pseudomonas.
The antibiotherapy was started with third-generation cephalosporins, Metronidazole, Vietnam, and maintained for 6 weeks, an antiepileptic and corticosteroid treatment was also prescribed.
The evolution of the patient was very impressive, fever and headache disappeared, the biological markers decrease seriously,
At least the patient had a gcs of 15 with no neurological deficit and was discharged 2 months after, fully recovered thanks to a combined surgical and antibiotic treatment.
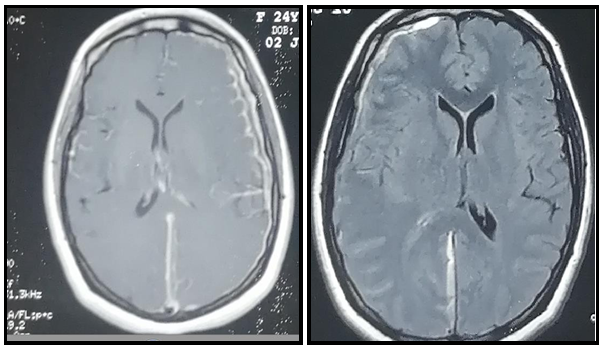
Figure 1: MRI shown the subdural empyema with midline shift
Discussion
Subdural empyema represents a loculated suppuration between the dura and the arachnoid It constitutes 15-25 % of all intracranial infections [2], the iatrogenic origin remains rare 1/12000 [1], and it may cause severe permanent neurological injury.
The most natural complaints are fever, headache, focal neurological signs, seizures. [3] The most common germ is Streptococcus, 82 % [4] but other germs could be found as mycoplasma hominins [5], enterobacter like our case.
MRI is the golden standard for diagnosis of subdural empyema, it shows the volume of the empyema, cerebral reaction as edema, hemorrhage, midline shift,ct scan can be very useful for bone analysis, and for regular control, also because of its availability [5] The treatment can be medical, surgical, or both, depending on the volume of the empyema, the clinical presentation of the patient, radiological findings,… the antibiotic should be adapted to the germ and maintained or changed depending on the evolution of the patient, the corticosteroid can also be associated, and in the most cases antiepileptic coverage is required.in case of a surgical treatment which is always combined with medical treatment, it let us evacuate the collection to get some samples for micro bacterial and histological analysis which is very precious for further treatment.
Our investigation, let us eliminate all the causes of fever, and it was considered as a postpartum fever, the theory supposes that a break in sterile technique happened during epidural anesthesia with the direct introduction of bacteria, this was facilitated by the immunodepression of the pregnant woman
However there are multiple ways for a microorganism to reach the central nervous system, as orl infection, endocarditis, acupuncture, so in our case, the spinal way remains only a supposition and we cannot completely rule out that this was the origin of the empyema.
Conclusion
The aim of our study is to underline the possibility of intracranial subdural empyema as a consequence of scpetic spinal anesthesia, physicians should be aware of this possibility in front of an explained postpartum fever, such complication could be easily avoided with more careful disinfection of instruments and puncture site. but Rapid diagnosis, correct evacuation, and an adapted antibiotic treatment can lead to perfect outcomes.
References
- Tovar IC, Alonso LG, Romero MC, Vergara LL, Heredia CMG, et al. (2019) Subdural Empyema by Streptococcus pyogenes after Epidural Anesthesia. Clin Case Rep Int. 3: 1118.
- Gençpınar P, Bektaş F, Aydın A, Duman M (2014) A Rare Cause of Fever: Subdural Empyema. The Journal of Pediatric Research. 1(3): 155-157.
- Schneeberger PM, Janssen M, Voss A (1996) Alpha-hemolytic streptococci: a major pathogen of iatrogenic meningitis following lumbar puncture. Case reports and a review of the literature. Infection. 24(1): 29-33.
- Calfee DP, Wispelwey B (1999) Brain Abscess, Subdural Empyema, and Intracranial Epidural Abscess. Curr Infect Dis Rep. 1(2): 166-171.
- Delgado Tapia JA, Galera López J, Santiago Martín J, Galdo Abadín JR, Quirante Pizarro A, et al. (2005) Subdural empyema due to Mycoplasma hominis after a cesarean section under spinal anesthesia. Rev Esp Anestesiol Reanim. 52(4): 239-42.