


Magna Condé1,2,3*, Aly Badara Nabé2, Loncény Fofana2, Mariame Camara2, Moussa Doré2, Aly Bernabé Ouendouno2, Norbert Traoré2
1African Center of Excellence for the Prevention and Control of Communicable Diseases (CEA-PCMT), Faculty of Health Sciences and
Techniques of the Gamal Abdel Nasser University of Conakry, Guinea
2Department of Odontology, Faculty of Health Sciences and Techniques, Gamal Abdel Nasser University of Conakry, Guinea
3Department of Odontology and Maxillofacial Surgery of the Ignace Deen National Hospital, Conakry, Guinea
4Department of Public Health of the Faculty of Health Sciences and Techniques, Gamal Abdel Nasser University Conakry, Guinea
*Corresponding Author: Magna Condé, Assistant and Teacher-Researcher at the Faculty of Health Sciences and Technology of the Abdel Nasser University of Conakry.
Abstract
Introduction: Medical accessibility is the ability of communities to access health services, both physically and in terms of cost, time, and availability by qualified personnel. This work aims to Contribute to the study of accessibility to oral care for the populations of the city of Siguiri.
Methods: This was a prospective descriptive study covering all consultants at the dental office of the Siguiri Hospital from March 1 to June 1, 2020.
Results: A total of 1024 patients were received in our department, including 400 who met our selection criteria, i.e., 39.06%. The age of our patients ranged between 18 and 87 years, with a mean age of 29 ± 10 years. The male gender was the most dominant (59.25%) and had a M/F sex ratio 1.45. Our series shows that 238 of our respondents were at their first consultation (60%), and those who had problems with access to oral and dental services were 231 patients (66%). 395, i.e., 98.75%, claimed to have used a means of transport. 49% of the territory's inhabitants should pay the cost of affordable care (67%). Nearly half of our respondents, or 43.86%, would have to wait 15 to 30 minutes before entering the treatment room.
Conclusion: Accessibility is essential for a qualified and efficient health system.
Keywords: Study, Accessibility, Oral care
Introduction
Accessibility is the ability of communities to access different health services, both physically and in terms of cost, time, and availability by qualified personnel. [1]. Availability and geographic accessibility assess the ease of access in time and space. In contrast, affordability and acceptability describe populations' socioeconomic characteristics and attitudes toward oral health service providers. These verbal health indicators will make it possible to focus the priorities of actions and educational programs and strengthen prevention and health needs. [3]. Many people in the world have problems accessing dental care [1]. Public health interventions to address these problems recognize that reducing inequalities in healthcare access is more accessible than reducing disparities in healthcare outcomes [10]. Thus, numerous studies carried out around the world [4,6,7,8,9] have shown that problems of accessibility to oral care are widespread and that their impact varies depending on the country, especially on policy. National health development. It therefore follows from all these studies that the solution to access to oral care is linked to the health system of each nation. The population of the city of Siguiri was 1,200,000 inhabitants, with only one public dental office available. People in the sub-prefectures have problems accessing oral care because of the distance separating them from the dental office. In addition, the condition of the roads in these sub-prefectures is poor. Most of the population must be made aware of medical treatment solutions for oral problems. Many people who need to be made aware of the medical treatment of dental issues need financial support to access the various therapies. The objective of this study is to contribute to the study of accessibility to oral care of the populations of the city of Siguiri, to describe the socio-demographic characteristics of the population, and to tell the factors of accessibility to oral care. Dental health of the population and to assess the cost of oral care
Materials and Methods
Type and duration of study
This prospective descriptive study took place in the city of Siguiri from March to June 2020 at the dental office of the Siguiri Prefectural Hospital.
Sampling technique
We conducted an exhaustive recruitment of 400 people among the 1024 who came for consultation at the dental office. Included in our study was any person aged 18 and over admitted to the service during the study period who agreed to give free and informed consent to participate in the study. The people whose general state of health did not allow them to provide the necessary time for our interview and those who did not give their free and informed consent to participate in the study were excluded.
Operational definition of variables
The different study variables described were quantitative (age) and qualitative (sex, profession, level of education, residence, type of treatment used, attendance at the oral and dental service, factors of accessibility to oral care, and attitude of the dentist.
Collection of data
Data was collected manually using a well-established survey form for this work. Data was captured, analyzed, and presented with EPI info in version 7.2.2.6 and using Word, Excel, and PowerPoint software from the 2013 office pack.
Data analysis
We carried out an analysis that described the characteristics of the sample using the median for quantitative variables and the proportion for qualitative variables.
Ethical considerations
The protocol of this study was approved by the scientific committee of the Department of Odontology of the Faculty of Health Sciences and Techniques of the Gamal Abdel Nasser University of Conakry and registered under the number 070/UGANC/2022 of the Rectorate. Informed consent from each patient or patient's parent was obtained before data collection.
Results
Our study involved 400 people who agreed to answer our questions. The average age was 29 ± 10 years old with extremes aged 18 – 87 years old with a predominance of those aged 18-37 years old, i.e., 45% (Table 1). The male gender was the most represented in the sample, i.e., 59.25% (Graph I), of which 27.75% were housewives (Table 2). Regarding educational level, people without schooling dominated, i.e., 51.25% (Table 3), and those living in rural areas were the most frequently encountered, i.e., 57.50% (Graph II). Concerning the type of treatment used, the modern one was predominant, i.e., 70% (Graph III). There were more people who had visited the dental office once (1) at 60% (Graph IV). As for accessibility to oral and dental services, people who did not have easy access to the dental office were the most encountered, i.e., 66.25% (Graph V). The most predominant nature of the accessibility problem was geographic, i.e., 86.66% (Graph VI). 98.75% of the population studied used transport to get to the hospital (Text 1). As for the distance travelled to access the dental office, greater than 15km is the most represented, i.e., 49% (Table 4). 99.25% of the population said they had the means to pay the cost of care (Text 2). About the cost of care, the population that benefited from an affordable price was by far the most encountered, i.e., 66.75% (Graph VII). The type of payment at the patient's expense dominated at 68% (Graph VIII). 99.25% of the study population answered yes to having the possibility of purchasing medications prescribed by the dentist (Text 3), and those satisfied with the waiting room were numerous, i.e., 94% (Graph IX). Concerning the waiting time before treatment, the people who waited between 15-30 min were the most encountered, i.e., 43.75% (Graph X), and the reassuring opinion on the attitude of the dental surgeon dominated, i.e., 51.50% (Graph XI). During our study, 99.74% of the population responded that they were satisfied with the quality of care received (Text 4). In this study, all dental surgeons confirmed the availability of access to care about the prevalence of oral and dental conditions (Text 5). During this study, 6 out of 7 dental surgeons stated that after informing patients about their pathologies (apart from the reason for the consultation) and drawing their attention to the need for treatment, they did not return for the execution. Care (Text 6). Distribution of patients received in consultation at the Siguiri prefectural hospital according to the execution of the treatment. Only 1/3 of our patients came for appointments (Text 7). Regarding patients' refusal to carry out treatment, the lack of interest in oral health is more noted, i.e., 50% (Table 6).
Table 1: Distribution of the study population according to Age
|
Age (Years) |
Numbers (n=400) |
Percentages (%) |
|
18 – 27 |
180 |
45.00 |
|
28–37 |
136 |
34.00 |
|
38 – 47 |
50 |
12.50 |
|
48 – 57 |
16 |
4.00 |
|
58 – 67 |
9 |
2.25 |
|
68 – 77 |
7 |
1.75 |
|
78 – 87 |
2 |
0.5 |
|
TOTAL |
400 |
100 |
Average age (29 ± 10 years) Extremes aged 18 – 87
Table 2: Distribution of the study population according to profession
|
Occupation |
Effective |
(%) |
|
Household |
111 |
27.75 |
|
Trader |
88 |
22.00 |
|
Worker |
70 |
17.50 |
|
Farmer |
55 |
13.75 |
|
Gold panner |
34 |
8.50 |
|
Official |
19 |
4.75 |
|
Pupil/Student |
23 |
5.75 |
|
Total |
400 |
100 |
Table 3: Distribution of the population according to level of education
|
Educational level |
Workforce |
Percentages (%) |
|
Not in school |
205 |
51.25 |
|
Primary |
69 |
17.25 |
|
Secondary |
105 |
26.25 |
|
Superior |
21 |
5.25 |
|
TOTAL |
400 |
100 |
Table 4: Distribution of the study population according to the distance traveled to access the dental office
|
Distance |
Workforce |
Percentages (%) |
|
˂ 5km |
135 |
34.00 |
|
5-10km |
20 |
5.00 |
|
10 - 15km |
50 |
13.00 |
|
> 15km |
195 |
49.00 |
|
TOTAL |
400 |
100 |
Table 5: Distribution of practitioners in the dental office of the Siguiri prefectural hospital according to patients' refusal to perform treatment
|
No renunciation of oral care |
Workforce |
(%) |
|
Difficult travel to get to the office |
1 |
16.66 |
|
Lack of interest in oral health |
3 |
50 |
|
Lack of motivation |
1 |
16.6 |
|
Fear |
1 |
16.6 |
|
Total |
6 |
100 |
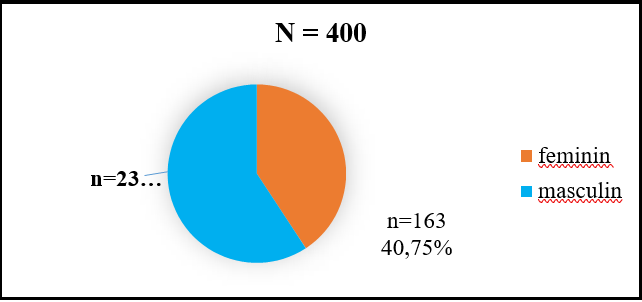
Chart I: Distribution of the study population according to sex
M/F sex ratio = 1.45
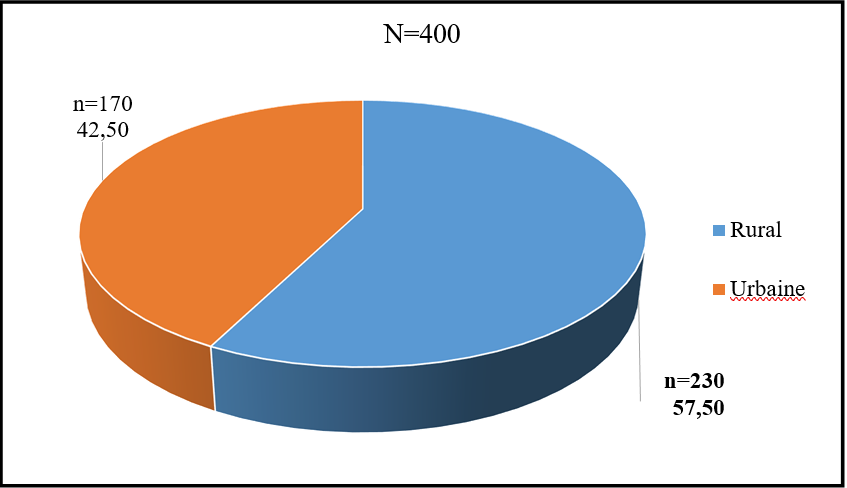
Chart II: Distribution of the population according to residence
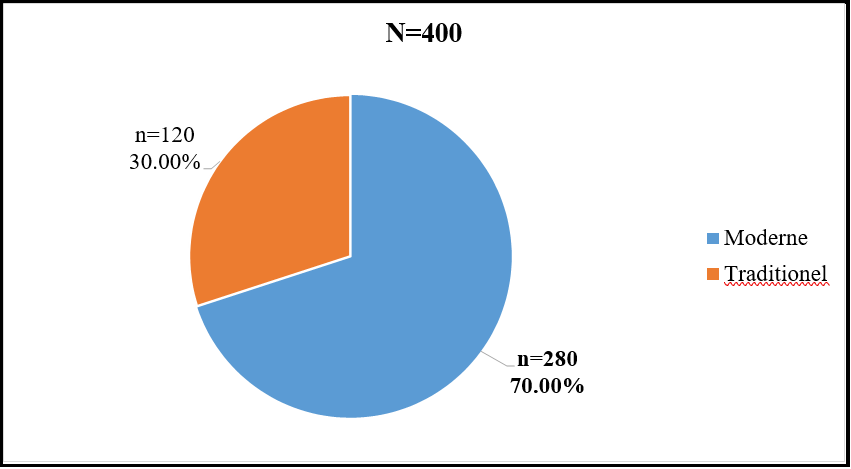
Chart III: Distribution of the study population according to the type of treatment used.
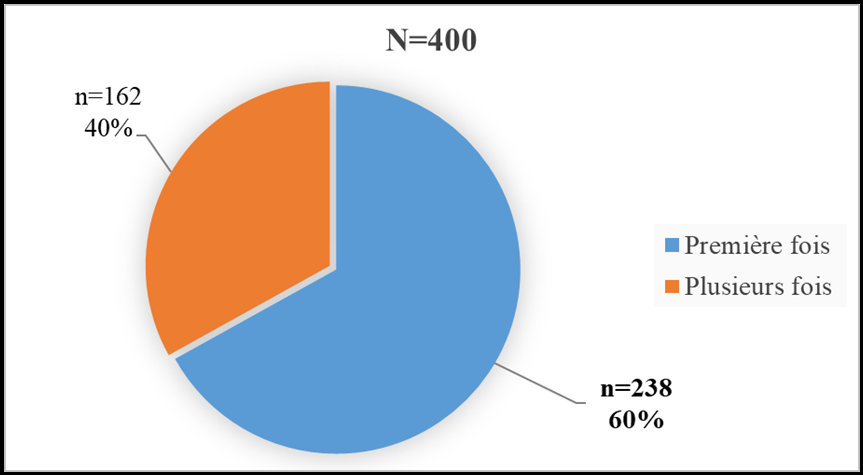
Chart IV: Distribution of the population seen in consultation at the dental office of the Siguiri prefectural hospital according to attendance at the service.
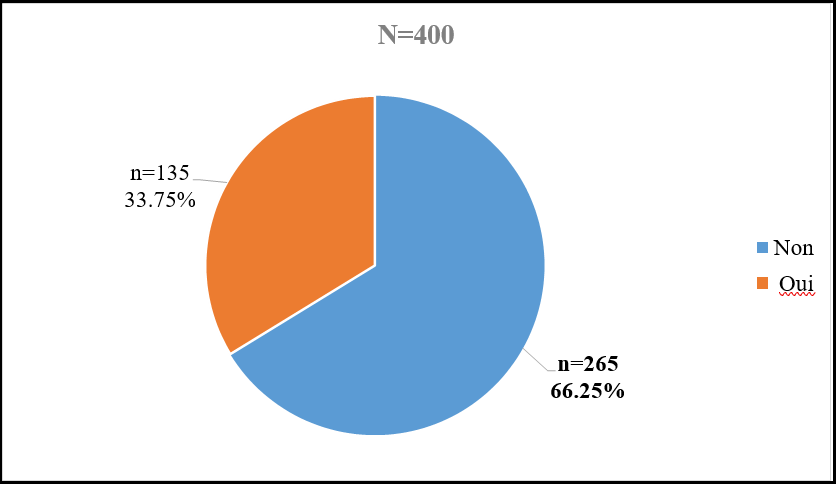
Chart V: Distribution of the study population according to accessibility to oral and dental services.
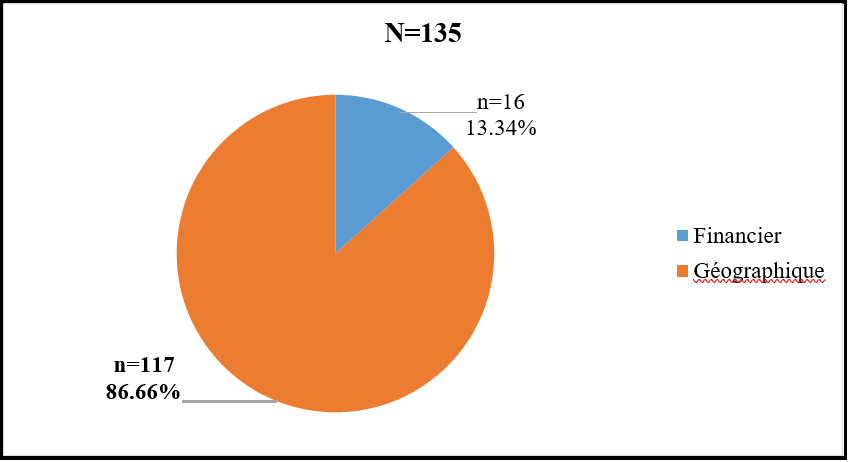
Chart VI: Distribution of the study population according to the nature of the accessibility problem encountered
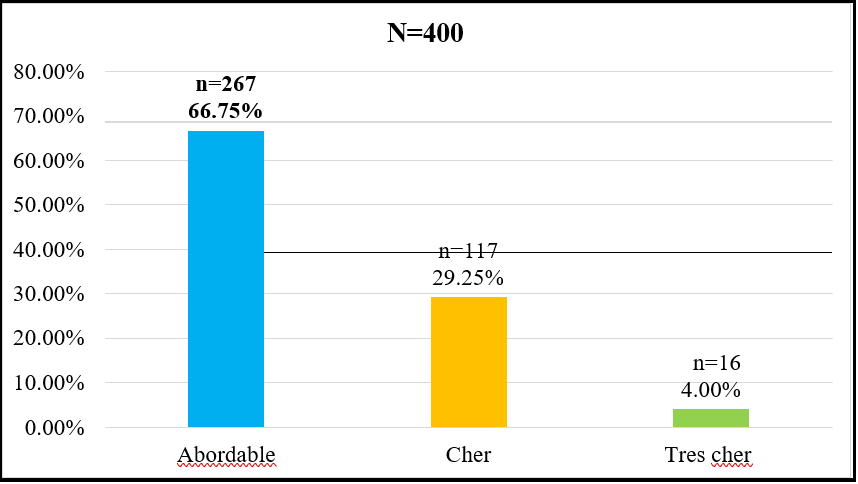
Graph VII: Distribution of the population seen in consultation at the dental office of the Siguiri prefectural hospital according to the cost of care
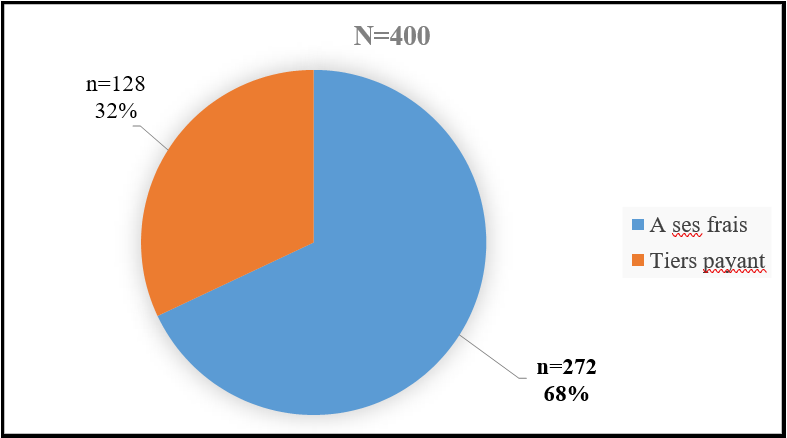
Chart VIII: Distribution of the population according to the type of payment.
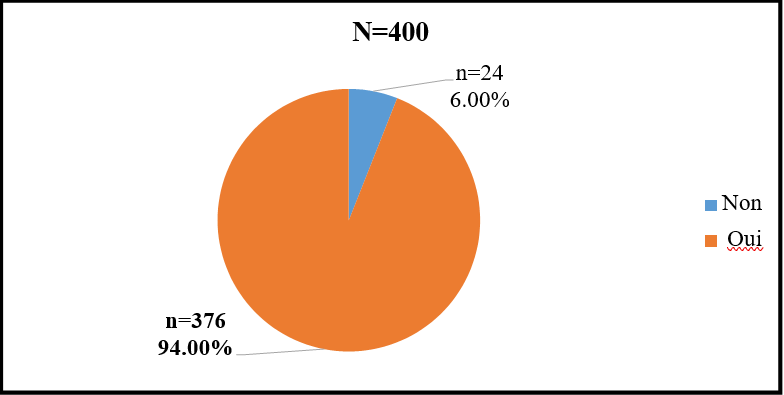
Chart IX: Distribution of the population according to their satisfaction with the waiting room.
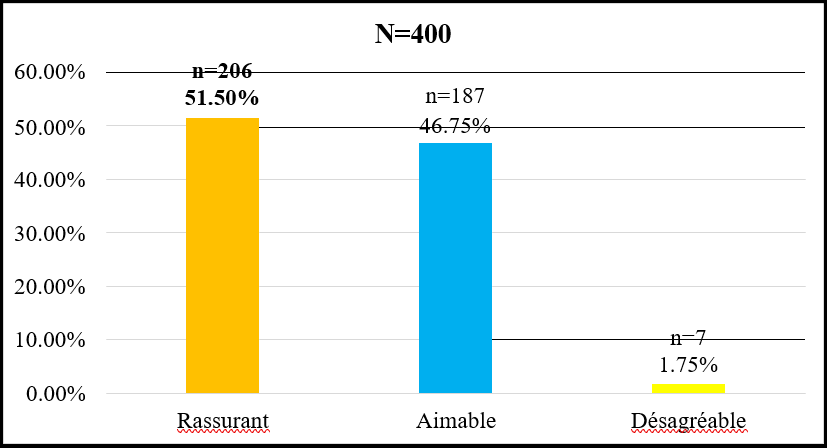
Chart XI: Distribution of the population according to their opinion on the attitude of the dentist
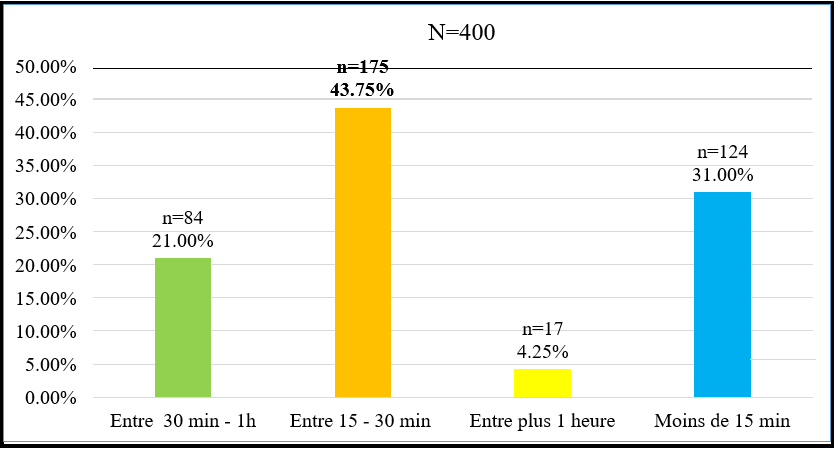
Graph X: Distribution of the population according to waiting time before entering the treatment room
Text 1: In our study, 395 or 98.75% of the population studied used a means of transport to go to the dental office of the Siguiri prefectural hospital compared to 5 or 1.25%.
Text 2: In this study, 397 or 99.25% of the population said they had the means to pay the cost care against 3 or 0.75%.
Text 3: In this study, 396, or 99.25% of the study population, responded yes to having the possibility of purchasing medications prescribed by the dentist compared to 3, or 0.75%.
Text 4: During our study, 396 or 99.74% Population responded that they were satisfied with the quality of care received compared to 1 or 0.25%.
Text 5: In this study, all dental surgeons confirmed the availability of access to care in relation to the prevalence of oral and dental conditions. Text 6: During this study, 6 out of 7 dental surgeons stated that after informing patients about their pathologies (apart from the reason for the consultation) and drawing their attention to the need for treatment, they did not return for the execution. care.
Text 7: Distribution of patients received in consultation at the Siguiri prefectural hospital according to the execution of the treatment. Only 1/3 of our patients came for the execution of appointments.
Discussion
Access to oral care is important because it is an integral part of general health and essential for well-being. However, its access is influenced by several factors [2]. Thus, during the three (3) months, 1024 people were registered in the service, among whom 400 agreed to answer our questions, i.e., 94.78%. This study allowed us to know the financial and geographical accessibility of the populations of Siguiri to oral care. However, the study should be conducted in the general population, which could not be done due to a lack of financial resources. The average age was 29 ± 10 years. The most represented age group was 18 – 27 years old, followed by 28 – 37 years old, with respective percentages of 45 and 34%. These results are close to those of Arwa et al. [21] in 2019 in Saudi Arabia, which reported a predominance of the age group of 18 – 24 years with 65%. On the other hand, our results are different from those of Tony B. et al. [22] In 2015, in Australia, the majority age group was 31 – 40 years old, with 30.8%. This high frequency among young people could be explained by the high representation of young people within the Siguiri population. Men were more represented with 59.25% compared to 40.75%, with a sex ratio of M/F=1.45. These results are similar to those of Salma AB et al. [23] In 2018, a male predominance of 53.8% was found in the south of Jeddah. On the other hand, these results differ from those of Tony B. et al. [22] in 2015 in Australia, which found a female predominance of 61.5%. The predominance of the male sex could be explained by the financial independence of men compared to women on the one hand, and men are more represented than women in the general presentation on the other hand. In this study, homemakers and traders were the most represented, with a percentage of 22 and 27.75%. Our results differ from those of Garé JV et al. [24] in 2019 in Burkina Faso, who reported a high frequency of unemployment at 35.3%. This could be explained by the fact that the prefecture of Siguiri is an artisanal gold mining zone where several for-profit activities are practiced, and the rate of immigration of homemakers from other prefectures or even from the sub-region of Siguiri is common. Those without schooling and those with secondary education were the most numerous, with 51.25 and 26.25%. Our results are close to those of Kanouté A. et al. [25] In 2015 Senegal, there was a predominance of non-schoolers at 62.7%. The influence of artisanal gold panning and commerce could explain the high frequency of out-of-school people. In this study population, 230 or 57.50% of our respondents resided in rural areas compared to 42.50% in urban areas. This proportion is different from that of Rodrigo M et al. [20] in 2017 in Chile, which reported a predominance of the urban population with 61.6%. On the other hand, it differs from that of Uguru N et al. [8] in 2020, Nigeria reported a rural population of 71.21%. The absence of adequate structures and qualified personnel for their care would justify this result. More than half of the respondents used modern treatment, i.e., 70%, compared to the traditional 30%. This rate is similar to that of Sangaré AD et al. [26] in 2017 in Ivory Coast, which reported 68.5% of modern treatment. This predominance of modern treatment could be explained by the failure of the treatment carried out by traditional practitioners. In this study, the majority of respondents were at their first consultation, with 238 or 60%. This result agrees with that of ABE K et al. [27] from 2004 to 2005, which reported 67%. This low rate of consultation for oral and dental services is due to ignorance and neglect of the consequences of a late dental consultation by communities. In this series, Most respondents had problems with access to oral and dental services, with 265 or 66.25% compared to 135 or 33.75%. These results are similar to those of Kanouté A et al. [25] in 2015 in Senegal, which reported 71.7%. The difficulty linked to accessibility is due to the number of structures offering dental consultations (a dental office for a population of nearly one million inhabitants), certain areas with difficult access, and the financial difficulty of certain patients to afford oral care services. In the sample, geographical problems (the distance patients travel to be at the dental office) were the most cited, with 86.66%. This proportion differs from that of the French Dental Association (ADF) in 2018[28]in France, which reported 15% geographical problems. This result could be explained by the poor road network in almost all rural areas. In this study, 98.75% of the population used a means of transport to go to the dental office of the Siguiri prefectural hospital compared to 1.52% who did not have a transport yen. The high frequency of use of means of transport has already been observed in studies conducted by Babacar D et al. [29] in 2005 in Senegal, which reported 70%. The use of means of transport would be due to the distance separating the dental service from the communities. In this study population, most respondents would have to travel more than 15 km and less than 5 km to get to the dental office of the Siguiri prefectural hospital, with 49 and 34%. These results are similar to those of Carbona FS et al. in 2018 in France [30], who reported that 60% of these respondents should do less than 5km. This result could be explained by the fact that most respondents came from rural areas that do not have dental care facilities and are, therefore, sometimes obliged to travel long distances to afford better care. The study sample points out that 99.25% of the population have the means to assume the cost of care compared to 0.25% who did not have the means and were not paid, which is not surprising all the more. that half (66.75%) believe that the services are affordable. Babacar D et al. [29], in 2005 in Senegal, reported that 56% of these respondents could not afford the cost of care. In this study, a large part of the respondents found the cost of care affordable at 66.75%. Unlike the work carried out by Faye D et al. [31] in 2012 in Senegal, who found that the cost of care was expensive, 70% of their respondents affirmed that the cost of care was expensive. This could be explained by the fact that the study was conducted in the hospital dental office, which is only frequented by people who can afford to be consulted. In this work, more than half of the respondents paid for the treatment at their own expense, with 272 or 68%. A study conducted by Sangaré AD et al. [32]in 2013 in Côte d'Ivoire reported a frequency of 98.7%. This result could be explained by the fact that the majority of patients surveyed are not insured. In this series, the respondents revealed the possibility of purchasing medications prescribed by the dentist at 99.25% compared to 0.25%. These results are similar to that of Uguru N et al. [8] in 2020 in Nigeria, who reported that 98% of their respondents said yes, they had the means to pay for medicines. This could be explained by the absence of mutual health insurance which supports patients in their care. In this work, almost all of the respondents were satisfied with the waiting room, with a percentage of 94. These results are comparable to that of Moustakim Y et al. [33] In 2018, they reported 88.9% of waiting room satisfaction in Morocco. Patient satisfaction with waiting is due to the good reception in the entrance office. Respondents would have to wait 15 to 30 minutes before being in the treatment room, i.e., 43.75%. Our results are different from those of Sangaré AD et al. [32] in 2013, Ivory Coast reported that 44.2% of their respondents would have to wait between 30 minutes and 1 hour before being taken into the treatment room. This is due to insufficient staff and equipment and the wait to disinfect certain instruments. In this study, 51.50% of respondents found the attitude of the dental surgeon reassuring. This result is lower than that of Kanouté et al. in 2015 in Senegal [25], who found a rate of 80.5%. This result could be explained by the fact that practitioners communicate well with patients during consultations. In this series, all patients were satisfied with the quality of care in 99.75%. Our results are higher than those of the French Dental Association (ADF) in France in 2018 [28], which reported 65% satisfaction. This could be explained by the dentist's attitude and the quality of care provided to the population. In this work, regarding forgoing oral care, practitioners stated that lack of interest in oral health was the main reason. Unlike the work carried out by Gérald M et al. [34] in 2017, France reported that fear was the ideal cause of 66%. The ignorance of most patients about the usefulness of oral health care could justify this result.
The main limitation of our study is the refusal or lack of interest of some people to participate.
Conclusion
Accessibility to oral care is a significant public health concern. The level of education and financial, physical, and geographic accessibility remain important determinants for using oral care in Siguiri. However, these results are part of improving accessibility to oral care for the populations of Siguiri prefecture. Consideration should be given to the establishment of a system of health coverage in general and oral and dental coverage in particular, with strong involvement of public authorities.
Author contributions
MC, ABN and MC participated in the design of the protocol. MC, NT, ABN, MD, LF, and ABO were involved in data acquisition, analysis, and interpretation. ABO, ABN MSF, MD and MAD reviewed the manuscript. All authors read, approved the final version and agreed to publication.
Data availability: Data regarding this study are available upon request from the authors.
Conflict of interest: The authors declare that they have no competing interests.
Funding: This study did not receive any funding from any public or private institution.
Thanks
The authors would like to thank the Faculty of Health Sciences and Technology, the CEA-PCMT, the CERFIG, the supervisors of the CEA-PCMT and the CERFIG of the Gamal Abdel Nasser University of Conakry for their unconditional contribution to the realization of this work.
References
- Alfaraj A, Halawany HS, Al-Hinai MT, Al-Badr AH, Alalshaikh M, et al. (2021) Barriers to Dental Care in Individuals with Special Healthcare Needs in Qatif, Saudi Arabia: A Caregiver's Perspective. Patient Prefer Adherence. 15: 69-76.
- Obeidat SR, Alsa'di AG, Taani DS (2014) Factors influencing dental care access in Jordanian adults. BMC Oral Health. 14(1): 127.
- Jin Z, Northridge ME, Metcalf SS (2018) Modeling the influence of social ties and transportation choice on access to oral healthcare for older adults. Appl Geogr. 96: 66‑76.
- Elani HW, Sommers BD, Kawachi I (2020) Changes In Coverage And Access To Dental Care Five Years After ACA Medicaid Expansion: Study examines changes in coverage and access to dental care five years after the ACA Medicaid expansion. Health Affiliate (Millwood). 39(11): 1900‑8.
- Eslamipour F, Heydari K, Ghaiour M, Salehi H (2018) Access to dental care among 15–64 year old people. J Educ Health Promot. 7(1): 46.
- author-kce. Geographic accessibility [Internet]. Towards a healthy Belgium. 2020.
- Abou Dramane Sangare. Oral health behaviors and determinants of healthcare use in the Dabou department - Ivory Coast [Doctoral thesis in medicine].[Ivory Coast]: Claude Bernard University - Lyon I; 2011.
- Uguru N, Onwujekwe O, Ogu UU, Uguru C (2020) Access to Oral health care: a focus on dental caries treatment provision in Enugu Nigeria. BMC Oral Health. 20(1): 145.
- Order of dental hygienists of Quebec. FOR BETTER ACCESSIBILITY TO PREVENTIVE ORAL CARE.Law 29 2019.
- Gondlach C, Catteau C, Hennequin M, Faulks D (2019) Evaluation of a Care Coordination Initiative in Improving Access to Dental Care for Persons with Disability. Int J Environ Res Public Health. 16(15): 27‑53.
- Sourzat L (2017) Odontology and developing countries: example of professional support at the dental office of the prefectural hospital of Siguiri, in Guinea Conakry [Internet] [exercise]. Toulouse III University - Paul Sabatier;.
- Ministry of Health and Public Hygiene. NATIONAL HEALTH DEVELOPMENT PLAN (PNDS) 2015-2024 [Internet]. Minister ofHealth ; 2015. Available on: National Health Development Plan 2015-2024 August 2015.pd
- The PDLGII development poles in Upper Guinea: a promising intercommunal socio-economic dynamic, an asset [Internet]. [Quoted June 21, 2021].
- National Institute Of Statistics Guinea. Final report: Census and mapping of basic socio-economic infrastructure in 2017. 2018.
- Galoula F (2017) Oral health indicators in children and the use of dental care in France [Internet] [Doctoral thesis in medicine]. [France]: PARIS DIDEROT UNIVERSITY - PARIS 7.
- author-kce. Accessibility of care [Internet]. Towards a healthy Belgium. 2019.
- Pascal BONNET. The concept of accessibility and access to care. [France]: Paul Valéry Montpellier 3 University; 20020.
- Clara Noirhomme. Access to health care, definition and issues. 2021;19.
- Evans DB, Hsu J, Boerma T (2013) Universal health coverage and universal access. Bull World Health Organ. 91(8): 546-546A.
- Mariño R, Giacaman RA (2017) Patterns of use of oral health care services and barriers to dental care among ambulatory older Chileans. BMC Oral Health. 17(1): 38.
- Alumran A, Almulhim L, Almolhim B, Bakodah S, Aldossary H, et al. (2019) Are dental care providers in Saudi Arabia prepared to treat patients with special needs? J Multidiscip Healthc. 12: 281‑90.
- Barnett T, Hoang H, Stuart J, Crocombe L (2017) The relationship of primary care providers to dental practitioners in rural and remote Australia. BMC Health Serv Res. 17(1): 515.
- Bahannan SA, Eltelety SM, Hassan MH, Ibrahim SS, Amer HA, et al. (2018) Oral and Dental Health Status among Adolescents with Limited Access to Dental Care Services in Jeddah. Dent J. 6(2): E15.
- Garé J, Kaboré W, Sawadogo A, Ouattara S, Fall M, et al. (2019) Late recourse to oral care in semi-urban areas in Burkina Faso: Knowledge and practices of populations on dental caries and its complications. Rev Col Odonto-Stomatol Afr Chir Maxillo-Fac. 26(4): 39-44.
- Kanouté A, Cisse D, Diouf M, Lô C, Faye D (2015) Acceptability of oral care among the elderly in Dakar (Senegal). Rev Col Odonto-Stomatol Afr Chir Maxillo-Fac. 22(3): 55‑9.
- Sangare AD, Samba M, Meless DG, Guinan JC, Bakayoko- LR, et al. (2013) Crossed perspectives on the use of modern and traditional oral care in Ivory Coast. Rev Col Odonto-Stomatol Afr Chir Maxillo-Fac. 20(3): 5‑11.
- ABE KOUTOUAN MATHURINE. accessibility to oral care: survey of 453 subjects in the dadou department. 2004 - 2005. Doctoral thesis. 183p [Doctoral thesis in medicine]. [IVOIR COAST]: University of ABIJAN; 2006.
- French Dental Association. access to dental care and coverage for dental prostheses. Dentaly.org; 2018.
- Diene B. Study of the accessibility of oral and dental care among the populations of the department of Thiès [Doctoral thesis in medicine]. [SENEGAL]: UCADD; 2005.
- Carbona Fadeuilhe S (2018) Inequalities in access to dental care and resolution solutions: example of Lot and Haute-Garonne [Internet] [exercise]. Toulouse III University - Paul Sabatier.
- Faye D, Kanouté A, Seck MT, Diouf AA. Accessibility to innovative healthcare technologies in Africa. Cah Public Health. 11(1): 54‑64.
- Sangare, AD, Samba, M, Guinan JCM, Diouf MJ, Bakayoko-Ly, et al. (2017) Socio demographic factors associated with renunciation to oral care in Ivory Coast. MOJ Public Health. 6(1): 241‑8.
- Moustakim Y (2018) Patients' perception of care services in the periodontology department [Doctoral thesis in dentistry]. [Morocco]: HASSAN II CASABLANCA UNIVERSITY.
- Maille G, Saliba-Serre B, Ferrandez AM, Ruquet M (2017) Use of care and the oral health status of people aged 60 years and older in France: results from the National Health and Disability Survey. Clin Interv Aging. 12: 1159‑66.