


Şenay Kurtulus MD
Department of Pediatric Surgery, Çanakkale Onsekiz Mart University Faculty of Medicine, Çanakkale, Turkey.
*Corresponding Author: Şenay Kurtulus MD, Department of Pediatric Surgery, Çanakkale Onsekiz Mart University Faculty of Medicine, Çanakkale, Turkey.
Abstract
Inguinal hernia is the most common surgical condition in childhood. Incarcerated inguinal hernia and strangulation of the sac contents are the most important and feared complications. Prematurity is estimated to be a risk factor for incarceration. In this study, a very premature baby weighing 1750 gms who was operated on for incarcerated inguinal hernia and strangulation is presented.
Keywords: Incarcerated inguinal hernia, prematurity,low-birthweight infant.
Introduction
Pediatric inguinal hernias are congenital and classified as indirect hernias based on the pathophysiology of the persistent processus vaginalis, which is associated with an increased risk of inguinal hernias in preterms. The incidence of inguinal hernia in children is 1- 5 %, and this rate may increase up to 30 % in premature babies. Approximately 60 % of inguinal hernias are right-sided, 30% are left- sided, and 10 % are bilateral. Boys are much more likely to have a hernia, with male-female ratios between 3:1 and 10:1 [1-3].
Incarceration is an important complication of inguinal hernias in children. The bowel, ovaries, or fallopian tubes are the organs that are most commonly incarcerated [4]. If the hernia does not regress spontaneously, the risk of incarceration is greatly increased. An incarcerated hernia can progress rapidly towards strangulation, a condition with vascular compromise and infarction of the incarcerated contents. Therefore, if an incarcerated hernia cannot be reduced manually, urgent inguinal exploration is required [4].
Case Reports
While the preterm baby was being followed up in the neonatal intensive care unit, he was consulted to the pediatric surgery department because of painful swelling in the right scrotum. It was stated that there was no swelling suggestive of a hernia since birth in the patient who was born at 28 weeks of gestation and had a very low birth weight (1000 gms). At the presentation, the baby with a postconceptional age of 36+2 weeks and a bodyweight of 1750 grams was restless and crying constantly. On physical examination, the right scrotum was edematous and tender.
In the ultrasonographic examination performed with the preliminary diagnosis of incarcerated inguinal hernia, herniated bowel loops were seen through a 4 mm defect from the inguinal canal to the right scrotal sac, and there was no peristaltic activity with increased echogenicity of the intestinal wall. With color Doppler, no obvious vascularity was observed in the intestine, and the proximal intestinal loops were dilated, thus these findings suggested strangulation.
With the diagnosis of an incarcerated hernia, he was taken to emergency surgery after the manual hernia reduction attempt failed. Thus, there was intestinal ischemia (Figure 1), but intestinal resection was not necessary, and the right testis circulation was also impaired (Figure 2). Following the application of warm saline, the intestinal circulation was restored and herniated loop was replaced in the abdomen along with high ligation of the herniated sac. The patient recovered completely after the operation. In the control ultrasonography 3 weeks later, the volume, shape, and parenchymal echogenicity of the affected right testis were similar to the contralateral normal testis, indicating that testicular atrophy did not develop.

Figure 1: Intraoperative view of the strangulated small intestine after inguinal exploration (white arrows).
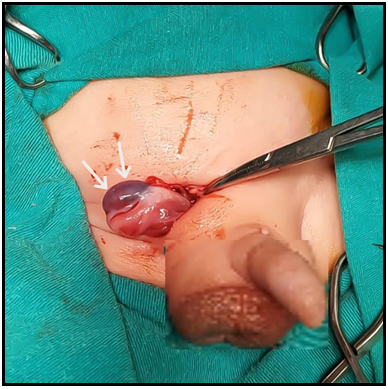
Figure 2: The purple appearance of the ischemic testis during the operation (white arrows).
Discussıon
The increase in survival rates of preterm infants with the contribution of advanced neonatal intensive care units is one of the reasons why inguinal hernia is more common in premature infants. Inguinal hernias often occur in the first year of life, and inguinal hernia repair is the most common surgical procedure performed by pediatric surgeons, and approximately one-third of children are younger than 6 months of age when they are operated on [1].
Management of inguinal hernia and timing of surgery is difficult in newborns with a hernia, especially in premature [5]. Hernia repair in premature infants is usually delayed until a certain weight or age is achieved in order to minimize the complications that may develop due to anesthesia, surgical technical difficulties, and comorbidities due to prematurity [6]. On the other hand, it is known that more than half of the premature with an inguinal hernia have been incarcerated, and the risk of incarceration doubles when the repair is delayed beyond 40 weeks of postconceptional age [6,7].
Those with very low birth weights have a 3-fold greater risk of requiring urgent procedures, resulting in higher recurrence rates and more complications, therefore elective hernia repair is recommended, especially in very low birth weight premature infants [8].
Although most pediatric surgeons prefer inguinal hernia repair before discharge, we think that even waiting until discharge from the hospital may increase the risk of unnecessary incarceration and therefore it should be operated on as soon as the diagnosis is confirmed [9,10].
Conclusion
The optimal timing for inguinal hernia repair in premature infants is important in balancing the risks of surgery and respiratory complications against complications such as strangulation. Inaddition, it should be kept in mind that the first appearance of an inguinal hernia may be by incarceration and should be considered in the differential diagnosis of sudden onset painful scrotal masses.
Consent for publication: Official consent received from the patinet.
Acknowledgments: None declared
References
- Grosfeld JL (1989) Current concepts in inguinal hernia in infants and children. World J Surg. 13(5): 506-515.
- Erdoğan D, Karaman I, Aslan MK, Karaman A, Cavuşoğlu YH (2013) Analysis of 3,776 pediatric inguinal hernia and hydrocele cases in a tertiary center. J Pediatr Surg. 48(8): 1767-1772.
- Morini F, Dreuning KMA, Janssen Lok MJH, Wester T, Derikx JPM, et al. (2021) Surgical Management of Pediatric Inguinal Hernia: A Systematic Review and Guideline from the European Pediatric Surgeons' Association Evidence and Guideline Committee. Eur J Pediatr Surg.
- Meena D, Jhuria R, Saxena S, Saini U (2017) Inguinoscrotal hernia in infants: Three case reports in ultrasound diagnosis. Indian J Radiol Imaging. 27(1): 78-81.
- Misra D (2001) Inguinal hernias in premature babies: wait or operate?. Acta Paediatr. 90(4): 370-371.
- Sulkowski JP, Cooper JN, Duggan EM, Balci O, Anandalwar SP, et al. (2015) Does timing of neonatal inguinal hernia repair affect outcomes?. J Pediatr Surg. 50(1): 171-176.
- Lautz TB, Raval MV, Reynolds M (2011) Does timing matter? A national perspective on the risk of incarceration in premature neonates with inguinal hernia. J Pediatr. 158(4): 573-577.
- de Goede B, Verhelst J, van Kempen BJ, Baartmans MG, Langeveld HR, et al. (2015) Very low birth weight is an independent risk factor for emergency surgery in premature infants with inguinal hernia. J Am Coll Surg. 220(3): 347-352.
- Crankson SJ, Al Tawil K, Al Namshan M, Al Jadaan S, Baylon BJ, et al. (2015) Management of inguinal hernia in premature infants: 10-year experience. J Indian Assoc Pediatr Surg. 20(1): 21-24.
- Verhelst J, de Goede B, van Kempen BJ, Langeveld HR, Poley MJ, et al. (2016) Emergency repair of inguinal hernia in the premature infant is associated with high direct medical costs. Hernia. 20(4): 571-577.