


Abdul Kader Mohiuddin
Secretary and Treasurer, Dr. M. Nasirullah Memorial Trust, Tejgaon, Dhaka 1215, Bangladesh
*Corresponding author: Mohiuddin AK, Secretary and Treasurer, Dr. M. Nasirullah Memorial Trust, Tejgaon, Dhaka 1215, Bangladesh
Abstract
Telemedicine and telehealth technologies are especially effective during epidemic outbreaks, when health authorities recommend implementing social distance systems. Currently, coronavirus COVID-19 has affected 210 countries around the world, killed nearly 170,000 and infected more than 2.4 million, according to worldometer, April 20, 2020. Home-care is especially important in these situations because hospitals are not seemingly safe during pandemic outbreaks. Also, the chance to get out of the home during the lockdown period is limited. Telephone- based measures improve efficiency by linking appropriate information and feedback. Tele-pharmacy allows to electronically share measurements of several parameters (e.g. blood pressure or BP, electrocardiograms or ECGs, blood lipids and glucose, body weight, etc.) and information on medications and life style behaviors among care givers and patients. It can also help provide education at distance on various health issues and topics. In addition to increasing access to healthcare, telemedicine is a fruitful and proactive way to provide a variety of benefits to patients seeking healthcare; diagnose and monitor critical and chronic health conditions; improve healthcare quality and reduce costs.
Abbreviations: IEDCR-Institute of Epidemiology, Disease Control and Research
Introduction
Bangladesh's health care services are becoming unusually concentrated in a small fraction of costly critical health-demanding patients. A large part of these complex-patients suffers from multiple chronic diseases and are spending a lot of money. Tele- pharmacy includes patient counselling, medication review and prescription review by a qualified pharmacist for the patients who are located at a far distance from the pharmacy. The most common way to use telemedicine is a responsive model, primarily physician-led with virtual visits stimulated by alerts using interactive services, which facilitates real-time interaction between the patient and provider [1]. It delivers resilience to services and enables pharmacists to work remotely, reducing the need for long journeys and increasing job satisfaction[2].The rise of pharmacists in epidemic situations has become increasingly popular in developed countries such as the United States, Australia, Canada and the United Kingdom. According to information from recent published articles in several ongoing journals, books, newsletters, magazines, etc., the duties, authority and responsibilities of pharmacists are completely different from doctors and nurses, although there are some similarities. Along with doctors, pharmacists can serve as frontline healthcare workers during epidemics. The profession is developed and highly praised in both developed and underdeveloped countries. Millions of professional pharmacists worldwide work in various organizations, and according to data from the International Pharmaceutical Federation (FIP), nearly 75% of them work in patient care [3]. Even in the United States, the continued lacking of primary health providers and medical specialists has made it possible for pharmacists to care for ambulatory patients with chronic diseases in a variety of treatment services [4].
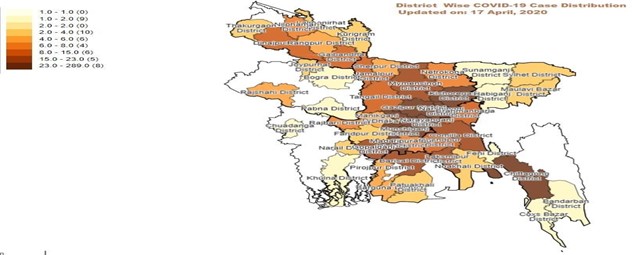
Figure 1: The Mapping of COVID-19 Confirmed Cases in BANGLADESH, 17 April 2020 (Source: IEDCR Web).
Methodology
Research conducted a month-round comprehensive literature search, which included technical newsletters, newspapers journals, and many other sources. The present study was started at the beginning of 2019. PubMed, ALTAVISTA, Embase, Scopus, Web of Science, and the Cochrane Central Register were thoroughly searched. The keywords were used to search for different publishers’ journals such as Elsevier, Springer, Willey Online Library, and Wolters Kluwer which were extensively followed. Medicine and technical experts, pharmaceutical company representatives, hospital nurses, and journalists were given their valuable suggestions. Projections were based on review of tele-pharmacists in both general and pandemic health situations, eligibility of pharmacists in telemedicine in general, present under-utilization scenario of Bangladeshi pharmacists in health services, let alone in telemedicine sector [5]. Major infrastructure revolution in both pharmacy education and country’s technological advancement are necessary to build an effective telemedicine system in this country.
Present Socio-Economic and Healthcare Situation
Bangladesh is the seventh most populous country in the world and population of the country is expected to be nearly double by 2050 [6], where communicable diseases are a major cause of death and disability [7]. A recent Dengue outbreak in 2019, more than 100,000 people was affected in more than 50 districts in Bangladesh in the first 6 months of 2019 [8,9]. According to World Bank's Country Environmental Analysis (CEA) 2018 report, air pollution lead to deaths of 46,000 people in yearly in Bangladesh [10]. Although a riverine country, 65% of the population in Bangladesh does not have access to clean water [11].Both surface water and groundwater sources are contaminated with different contaminants like toxic trace metals, coliforms as well as other organic and inorganic pollutants [5]. Studies in capital Dhaka and Khulna also found that about 80% of fecal sludge from on-site pit latrines is not safely managed [12]. Nearly half of all slum dwellers of the country live in Dhaka division [13] and 35% of Dhaka's population are thought to live in slums [14]. A recent research demonstrates widespread poor hygiene and food-handling practices in restaurants and among food vendors [15].Less than 10% hospitals of this country follow the Medical Waste Management Policies [16]. In 2017, 26 incidents of disease outbreak were investigated by National Rapid Response Team (NRRT) of IEDCR [17].Economic development and academic flourishment do not represent development in health sector. Out of the pocket treatment cost raised nearly 70 % in the last decade [18].Although, officially 80 % of population has access to affordable essential drugs, and there is plenty of evidence of a scarcity of essential drugs in government healthcare facilities [19]. Surprisingly, the country’s pharmaceutical sector is flourishing, exports grew by more than 7% in last 8 months although total export earnings of the country drop to nearly 5%[20]. It has been found in Bangladesh that more than 80% of the population seeks care from untrained or poorly trained village doctors and drug shop retailers [21]. According to WHO, the current doctor-patient ratio in Bangladesh is only 5.26 to 10,000, that places the country at second position from the bottom, among the South Asian countries [22]. According to World Bank data, Bangladesh has 8 hospital beds for every 10,000 people; by way of comparison, the US has 29 while China has 42 [23]. Tobacco is responsible for 1 in 5 deaths in Bangladesh, according to the WHO, kills more than 161,000 people on average every year. Around 85% population of age group 25-65 never checks for diabetes [24,25].
Pharmacy Education in Bangladesh
Pharmacy Education in many developing countries, including Bangladesh, is still limited to didactic learning that produce theoretically ‘skilled’ professionals with degrees. Pharmacy curriculum in Bangladesh do not satisfy the minimal requirement for appropriate education in clinical, hospital and community pharmacy, since they are still linked to an old model of pharmacy activity e.g. based on chemistry and basic sciences. That is present curriculum produces Pharmacist only to work in the pharmaceutical industry and jobs in this field of work is going to be saturated. No university so far has modified their curriculum including topics as epidemiology, pharmaco-economics, clinical medicines, community skills. Manpower development for community pharmacies in Bangladesh is not systematically regulated and constitutes an important public health issue. Three levels of pharmacy education are currently offered in Bangladesh leading to either a university degree, a diploma or a certificate. Graduates with degrees work in industry while those with diplomas work in hospitals [26]. Pharmacy is taught in about 100 public and private universities in Bangladesh and about 8000 pharmacy students graduate every year [27].Hospital, community and clinical pharmacy in Bangladesh have not been well developed due to lack of government policy [28]. In real conditions of Bangladesh pharmacy practice areas for graduate pharmacist is limited in industry i.e., industrial pharmacy practices, in the marketing or regulatory sections. The educational system of pharmacy is one of the major reasons for bounded pharmacy practices because the courses included in bachelor degree principally emphasize on industrial practices [29]. Over 90% of B. Pharm curriculum emphasizes on product-oriented knowledge whereas only around 5% of the total course credits are allocated toward clinical pharmacy. This curricular framework indicates a minimum emphasis on patient care education [30]. However, the graduates who pass out do not get employment easily due to their poor training, lack of in-depth knowledge of fundamental concepts and practical skills [17]. Consequently, skilled graduates leave for overseas where they find more prosperous jobs. Researchers argued that Pharmacy Education can be able to contribute for both public and private benefits if a realistic pattern is ensured on its operation [31]. This system could be more beneficial to the public if the good hospital and community practices are introduced properly and also by involving the pharma professionals e.g. pharmacists and other skilled health care providers.
Present State of Pandemic Situation Handling by Bangladeshi Hospitals
Nearly half of the 2948 coronavirus cases detected in Bangladesh have been reported in the capital Dhaka[32]. The virus hit a total of 11 out of the 64 districts in the country until 05.04.2020 after the first known cases were reported around a month ago, according to the government’s disease control agency IEDCR [33]. Amidst this global crisis, Bangladesh has been identified as one of the 25 most vulnerable countries to be affected by the fast-spreading virus. From 1st April to 14th, Covid-19 cases became 20- fold and by 20.04. 2020, it was confirmed in 53 districts [34,35]. Many patients with fever, cold and breathing problems – which are also COVID-19 symptoms – have gone untreated as the hospitals in Dhaka are sending them to the IEDCR for coronavirus test [36]. Many doctors are not providing services fearing the contagion and lab technicians are shunning workplaces halting medical tests, according to the patients. In some cases, serious patients who are not affected by COVID-19, moved from one hospital to the other but could not receive treatment and finally died, the media reported. In another case, the doctor fled leaving the patient behind [37- 40].Doctors and other healthcare workers say they do not have adequate personal protective equipment and the health system cannot cope with the outbreak [41]. Police have locked down a total 52 areas of Dhaka after Covid-19 positive patients were found in the localities [42].Experts say elderly people infected with coronavirus need ICU support the most. The number of older persons in the country is over 0.8 million [43]. The country's entire public health system has less than 450 ICU beds, only 110 of which are outside the capital Dhaka [23].The economic shutdown sparked by COVID-19 threatens millions of livelihoods in the country imminently. Law enforcers have been struggling to enforce shutdown and keeping people confined to their homes but people often ignored their request and instructions [44].
Under Utilization of Hospital Pharmacy
The pharmacy profession is still lagging behind in developing countries as compared with developed countries in a way that the pharmacy professionals have never been considered as a part of health care team neither by the community nor by the health care providers. Although hospital pharmacists are recognized for its importance as health care provider in many developed countries, in most developing countries it is still underutilized or underestimated [45-48]. Hospital pharmacy practice is just started in some private modern hospitals in Bangladesh which is inaccessible for the majority of peoples due to high patients cost of these hospitals [49]. People are totally unknown to the responsibilities of hospital pharmacist, even they don’t seek for recruit for hospital pharmacist in any hospital except a few aristocrat hospitals [50].A survey in Dhaka reported that 48% of respondents with symptoms of acute respiratory illness (ARI) identified local pharmacies as their first point of care. Licenses are provided to drug sellers by the Directorate General of Drug Administration when they have completed a grade C pharmacy degree (i.e. 3 months course) to legally dispense drugs[51] but a grade A pharmacy degree holder, having a B.Pharm or Pharm. D degree should be more equipped to handle these situations, if trained properly. Knowledge and helpfulness of pharmacist were identified as two major determinants that could not only satisfy and but also promote willingness to pay for the service [52]. They can individualize the medications and their dosing according to the needs of the patient, which can minimize the cost of care for the medication. In Bangladesh, however, graduate pharmacists do not engage directly in-patient care. Here, pharmacies in hospitals are primarily run by non-clinically educated, diploma pharmacists [28]. If the hospital pharmacy is established, patient care, proper dispensing of medications, and other patient-oriented issues can be handled properly. By maintaining a hospital pharmacy quality control program, the health sector can be enriched.
Prospect of Pharmacists in Patient Management Service and Telehealth Care
Pharmacists are the third largest healthcare professional group in the world after physicians and nurses [53]. At present, Hospital Pharmacy has created enormous job opportunities, where graduate pharmacists play a vital role in patient rearing, rehabilitation and wellness. A professional pharmacist or a pharmacy apprentice at a clinic, hospital and community care can determine what to do in a given disease situation, if guided properly by another medical personnel [54-56]. The country has a huge opportunity to recruit these pharmacists at Telehealth Care. In each call, a pharmacist can provide both appropriate and quality information from the most recent medical systems. Studies show that the lack of proper medication management leads to higher healthcare costs, longer hospital stays, morbidity and mortality. Further, it was reported that one in every five hospitalizations was related to post- discharge complications and about seventy percent were related to proper use of the drug. In 2017, the World Health Organization committed to minimizing serious, avoidable drug-related harm over the next 5 years. Pharmacists' interventions to prevent drug- related problems at three community hospitals in California saved approximately 0.8 million USD in a year [57]. The estimated annual cost of medication error-based illnesses and deaths worldwide was USD 500 billion due to non-compliance with the clinical intervention and quantities in 2016. Also, the authors estimate that more than 275,000 people die every year for the same reasons [58]. A pharmacist can use simple and non-medical terminology to set the goal for patients to understand the information as well as to fulfill the prescription by proper request. With chronic conditions such as cardiovascular and respiratory diseases, there is ample evidence of the effectiveness of the tele-pharmacist for remote monitoring, communication and consultation [59]. In addition, psychotherapy can also be operated through telehealth as part of behavioral health [60]. The pharmacy-related needs of pandemic patients have similarities with the traditional patient population, but with different emphasis [61]. For example, when providing consulting services to patients, instead of focusing on medications as usual, their queries relate primarily to the knowledge of medical prevention and basic details on COVID-19, such as mask selection and standard COVID-19 signs and symptoms, symptomatic treatment options, breathing difficulties or cough management in comorbid situations, reinforcing behaviors that limit the spread of the pandemic, including social distancing and remaining in the home whenever possible through phone calls/video conferencing[62,63]. Earlier, Student pharmacists served as an effective education resource for patients regarding the H1N1 pandemic [64]. Sorwar et al. 2016 revealed that the existing telemedicine service reduced cost and travel time on average by 56 % and 94 % respectively compared to its counterpart conventional approach with high consumer satisfaction [65].
History of Telehealth Service in Bangladesh
The year 1998 is a milestone for eHealth in Bangladesh since Swinfen Charitable, a not-for-profit institution, launched the first eHealth project. It involved a collaboration between the Bangladesh Center for Paralyzed Rehabilitation (CRP) and the Haslar Royal Navy Hospital, in the UK. The Ministry of Health and Family Welfare (MoHFW) launched its first eHealth initiative in the same year [66,67]. Just a year later the private company Telemedicine Reference Center Limited (TRCL) started using mobile phones to deliver healthcare. A professional coalition, the Bangladesh Telemedicine Association (BTA) was created in 2001. That provided a platform for the country's ongoing and sporadic eHealth initiatives. A similar platform was formed in 2003, called the Sustainable Development Network Program (SDNP), with the aim of establishing better collaboration and understanding between providers [68]. Later in 2006, TRCL paired with Grameenphone (GP) and established a subscriber mobile phone call center called Health Line: 789 [69,70]. A number of NGOs, including BRAC, Sajida Foundation and DNet subsequently developed an interest in eHealth and mHealth [71]. Additionally, Bangladesh launched a toll-free national emergency helpline 999 for immediate needs in the case of any accident, crime, fire or ambulance in December 2017 [72]. Besides, there are 17 hotline numbers that were launched by the IEDCR [73].
Challenges of Tele-pharmacy Implementation
First, it has limited evidence of its efficacy beyond that of a traditional pharmacist’s intervention. These favor both doctors’ and patients’ skepticism towards these services and limits their diffusion in the community [74]. Second, the tele-pharmacy is a service based on the technology. Thus, the driver is technology but also the limiting factor for its implementation. Establishing a tele-pharmacy service involves not only meeting technological requirements but also a considerable amount of time, effort and money [75]. Third, effective tele-pharmacy services should be based on standardized models of healthcare provision and need appropriate regulations that may differ from one country to another. For example, in some countries such services are not permitted or even prohibited, while in others such as the USA, Italy and other European countries appropriate legislation is available [76-79]. Unfortunately, in many countries, despite the widespread potential of tele-pharmacy, the laws and policies that govern pharmacy operations do not adequately address the growing industry. Fourth, reluctance or inability to use modern technologies may limit the implementation of tele-pharmacy services both from the pharmacist’s and patient’s perspective, particularly in case of elderly people [80-85]. Fifth, since tele-pharmacy involves collecting, transmitting and replacing personal and health information on the Internet, security and privacy of information is a major issue. Data sharing of information collected with other healthcare professionals through tele- pharmacy services increases the risk of security breaches. The security and integrity of patient data is therefore of paramount importance when determining the setup of a tele-pharmacy system of information technology [86-91]. Sixth, the integration of tele- pharmacy services in the national healthcare systems and the connection of tele-pharmacy services (including a combination of electronic data entry, prescription order verification, online benefit adjudication, medication dispensing) among different areas of a country requires harmonizing the healthcare systems and related governing laws and setting up proper rules and regulations[92-94]. Seventh, tele-pharmacy services are not yet reimbursed: individuals have to pay for these services and the expenditures are not covered by private or public health insurances [95-99]. This limits the use of these services by patients eventually needing them.
Overcoming Challenges
In Bangladesh a number of telemedicine systems were introduced. Telemedicine laws and reimbursement policies since telemedicine practice is increasing on a daily basis in Bangladesh, so structured laws and regulations on doctors, patient issues, licensing of physicians and telemedicine providers are very much needed. Clear rules should be in place on questions of reimbursement. Bangladesh Television (BTV) and other satellite channels can play an important part in popularizing telemedicine. They should broadcast successful cases considering telemedicine's efficacy and cost- efficiency. Telemedicine systems and services compatibility of hardware and software require users to have compatible hardware at both ends of the communications link, which reduces interoperability and the benefits of access to different sources of telemedicine expertise. If the equipment is difficult to access or are less likely to involve practitioners. Equipment for wireless telemedicine is preferable to wire devices. Telemedicine privacy and confidentiality involves the electronic transmission of patient medical records and information from one location to another via the Internet, or other computerized media. Medical information is often delicate, confidential and private. Tele medicine, thus presents significant challenges for safeguarding the privacy and confidentiality of information about patient health. Specific privacy regulations should govern the practice of telemedicine so that patients can feel safe in knowing that confidentiality of their personal information will have to suffer certain penalties.
Conclusion
Overburdened by patient loads and the explosion of new drugs, physicians turned to pharmacists more and more for drug information, especially within institutional settings. They obtain medical and medication history, check medication errors including prescription, dispensing and administration errors, identify drug interactions, monitor ADR, suggest individualization of dosage regimen, provide patient counseling, etc. Among chronic disease patients, particularly those under quarantine, there is a greater challenge in the supply of drugs and compliance with medications, although the safety and effectiveness of care is still critical for these patients. Stronger data on the effectiveness of this area of pharmacy care, together with a critical assessment of its limitations, can raise awareness among the actors involved about its potential and could contribute to a wider dissemination of tele-pharmacy services in public interest.At the end, it can be said that pharmacists can play a role in both medical aids and regulation. But their social acceptance as a frontline patient care provider is necessary first. Similarly, in tele-healthcare, the professional pharmacist can play an essential role that has not been recognized yet due to lack of proper initiatives. We hope that policy makers of Bangladesh are aware of its potential and contribute to the wider promotion of tele-pharmacy services in the interest of the citizenry.
Acknowledgement
I’m thankful to Dr. Colin D. Rehm, Clinical Assistant Professor, Department of Epidemiology & Population Health, Alert Einstein College of Medicine, NY, USA for her precious time to review my literature and thoughtful suggestions. Also, I’m also grateful to seminar library of Faculty of Pharmacy, University of Dhaka and BANSDOC Library, Bangladesh for providing me books, journal and newsletters.
Financial Disclosure or Funding: N/A
Conflict of Interest: The author declares that he has no competing interests.
References
- Kane-Gill SL, Niznik JD, Kellum JA (2017) et al. Use of Telemedicine to Enhance Pharmacist Services in the Nursing Facility. Consult Pharm 32 (2): 93-98.
- Pike H (2018) Web therapy: how pharmacists are leading the way on telehealth. The Pharm J.
- Bates I, John C, Bruno A, Fu P, Aliabadi S (2016) An analysis of the global pharmacy workforce capacity. Hum Resour Health 14(1): 61.
- Goode JV, Owen J, Page A, Gatewood S (2019) Community-Based Pharmacy Practice Innovation and the Role of the Community- Based Pharmacist Practitioner in the United States. Pharmacy (Basel) 7(3): 106.
- Hasan MK, Shahriar A, Jim KU (2019) Water pollution in Bangladesh and its impact on public health. Heliyon 5(8): e02145.
- Saha S, Hossain MT (2017) Evaluation of medicines dispensing pattern of private pharmacies in Rajshahi, Bangladesh. BMC Health Serv Res 17(1): 136.
- Muhammad F, Chowdhury M, Arifuzzaman M, Chowdhury AA (2017) Public Health Problems in Bangladesh: Issues and challenges. South East Asia J Pub Health 6(2): 11-16.
- Dayaram S, Pokharel S (2017) Bangladesh hit by worst dengue outbreak on record. CNN health.
- Mohiuddin AK (2019) Dengue Epidemic Situation in Bangladesh. Journal of Clinical Case Studies 4 (3).
- Mohiuddin AK (2019) Chemical Contaminants and Pollutants in the Measurable Life of Dhaka City. Eur J Sus Dev Res 3(2).
- BBS/UNICEF Bangladesh MICS 2012-2013 Water Quality Thematic Report, March, 2018.
- Amin N, Rahman M, Raj S, et al. (2019) Quantitative assessment of fecal contamination in multiple environmental sample types in urban communities in Dhaka, Bangladesh using Sani Path microbial approach. PLoS One 14(12): e0221193.
- AlShoaibi AAA, Matsuyama A, Khalequzzaman M, Shahjahan Ali,Jamie Green, et al. (2018) Perceptions and behavior related to noncommunicable diseases among slum dwellers in a rapidly urbanizing city, Dhaka, Bangladesh: a qualitative study. Nagoya J Med Sci 80(4): 559-569.
- van der Heijden J, Gray N, Stringer B, Aminur Rahman, Sadika Akhter, et al. (2019) 'Working to stay healthy', health-seeking behaviour in Bangladesh's urban slums: a qualitative study. BMC Public Health19(1): 600.
- Nizame FA, Alam MU, Masud AA, Shoab AK, Opel A, et al. (2019) Hygiene in Restaurants and among Street Food Vendors in Bangladesh. Am J Trop Med Hyg 101(3): 566-575.
- AK Mohiuddin (2018) Medical Waste: A Nobody’s Responsibility After Disposal. Int J Environ Sci Nat Res; 15(2): 555908.
- Mohiuddin A (2019) An A-Z Pharmaceutical Industry: Bangladesh Perspective. Asian JResPharm Sci 9(1):17-28.
- Mohiuddin AK (2019) Pharmaco-economics: Essential but merely practiced in Bangladesh. Academia Journal of Scientific Research; 7(3): 182-187.
- Husain M, Rahman M, Alamgir A, Uzzaman MS, Flora MS (2019) Disease Surveillance System of Bangladesh: Combating Public Health Emergencies. Online J Public Health Inform11(1):e334.
- Online Report. Export earnings drop to $26.24b in eight months. The Financial Express, March 05, 2020.
- Ahmed SM, Naher N, Hossain T, Rawal LB (2017) Exploring the status of retail private drug shops in Bangladesh and action points for developing an accredited drug shop model: a facility based cross-sectional study. J Pharm Policy Pract 10:21.
- Mohiuddin AK (2020) Patient satisfaction with healthcare services: Bangladesh perspective. International Journal of Public Health Science (IJPHS) 9(1):34-45.
- Saleh A. In Bangladesh, COVID-19 threatens to cause a humanitarian crisis. World economic Forum.
- Mohiuddin AK (2019) TRACK (by NEHEP) Implementation: A Bangladesh Scenario. PharmacovigPharmacoepid2(1):28-36.
- Mohiuddin AK (2019) Diabetes Fact: Bangladesh Perspective. International Journal of Diabetes Research; 2(1): 14-20.
- Alam G, Shahjamal M, Al-Amin A, Azam M. (2014) State of Pharmacy Education in Bangladesh. Tropical Journal of Pharmaceutical Research; 12 (6): 1106.
- Mazid MA, Rashid MA (2011) Pharmacy Education and Career Opportunities for Pharmacists in Bangladesh. Bangladesh Pharmaceutical Journal;14 (1): 1-9.
- Saha T, Bhuiya RH, Masum ZU, Islam MR, Chowdhury JA (2018) Hospital Pharmacy Management System and Future Development Approaches in Bangladeshi Hospital. Bangladesh Pharmaceutical Journal; 20(2): 180- 187.
- Jakaria M (2015) Pharmacy practices in Bangladesh. The Independent/Stethoscope.
- Islam MA, Gunaseelan S, Khan SA, Khatun F, Talukder R (2014) Current challenges in pharmacy education in Bangladesh: A roadmap for the future. Currents in Pharmacy Teaching and Learning; 6(5): 730-735.
- Alam GM, Al-Amin AQ (2014) Role of Pharmacy Education in National Development of Bangladesh: A Scope for Public and Private Sectors. Indian Journal of Pharmaceutical Education and Research; 48 (4):11-21.
- Maswood MH (2020) Bangladesh COVID-19 death tops 100. NEWAGE Bangladesh.
- Senior Correspondent. Coronavirus cases detected in 11 districts, more than half of them in Dhaka. bdnews24.com.
- Nabi MS (2020) Shovon FR. 20-fold rise in Covid-19 cases in Bangladesh since April 1. DhakaTribune, April 14.
- Staff Reporter. 11 districts remain coronavirus free. The New Nation, April 21, 2020.
- The Financial Express. Entire Bangladesh is at risk: Health Directorate. National, 16 April, 2020.
- Masum O. Dhaka hospitals turning away patients with fever, cold needing coronavirus tests. bdnews24.com, 19.03.2020.
- Staff Correspondent. Health minister vows to punish private hospitals for turning away patients. bdnews24.com, 03.04.2020.
- Islam Z, Mollah S. Admission to Hospitals: Patients left in quandary. The Daily Star, 24.03.2020.
- Akhter F. COVID-19 and healthcare denial. NEWAGE OPINION, 02.04.2020.
- UNB. DU student ‘denied treatment by hospitals’ dies. The Financial Express/National, 07.04.2020. 42.
- Chowdhury T. Poor Bangladeshis being turned away from hospitals. Al Jazeera America News/Bangladesh, 07.04.2020.
- Tribune Report. Police lock down 52 areas in Dhaka. DhakaTribune, 08.04.2020.
- Tajmim T. Bangladesh has only 29 ICU beds to fight coronavirus! The Business standard, 24.03.2020.
- Mahmud I. Bangladesh police struggle enforcing pandemic shutdown. NEWAGE Bangladesh, April 11,2020.
- Azhar S, Hassali MA, Ibrahim MI, Ahmad M, Masood I, Shafie AA (2009) The role of pharmacists in developing countries: the current scenario in Pakistan. Hum Resour Health; 7:54. Published 2009 Jul 13.
- Sakeena MHF, Bennett AA, McLachlan AJ (2018) Enhancing pharmacists' role in developing countries to overcome the challenge of antimicrobial resistance: a narrative review. Antimicrob Resist Infect Control. May 2; 7:63.
- Sakeena MHF, Bennett AA, McLachlan AJ. The Need to Strengthen the Role of the Pharmacist in Sri Lanka: Perspectives. Pharmacy (Basel). 2019; 7(2): 54. Published 2019 Jun 5.
- Rayes IK, Hassali MA, Abduelkarem AR (2015) The role of pharmacists in developing countries: The current scenario in the United Arab Emirates. Saudi Pharm J; 23 (5): 470–474.
- Paul TR, Rahman MA, Biswas M, Rashid M, Islam MAU (2015) Practice of Hospital Pharmacy in Bangladesh: Current Perspective. Bangladesh Pharmaceutical Journal; 17(2): 187- 192.
- The Pharmaceutical Journal. Development of Hospital Pharmacy in Bangladesh. News & analysis, June 01, 2009.
- Chowdhury F, Sturm-Ramirez K, Mamun AA et al (2017). Factors driving customers to seek health care from pharmacies for acute respiratory illness and treatment recommendations from drug sellers in Dhaka city, Bangladesh. Patient Prefer Adherence; 11: 479–486.
- AlShayban DM, Naqvi AA, Islam MA et al (2020). Patient Satisfaction and Their Willingness to Pay for a Pharmacist Counseling Session in Hospital and Community Pharmacies in Saudi Healthcare Settings. Front Pharmacol; 11:138.
- Khan AN, Khan MU, Shoaib MH, Yousuf RI, Mir SA (2014) Practice nurses and pharmacists: a perspective on the expectation and experience of nurses for future collaboration. Oman Med J; 29(4): 271–275.
- Jorgenson D, Dalton D, Farrell B, Tsuyuki RT, Dolovich L (2013) Guidelines for pharmacists integrating into primary care teams. Can Pharm J (Ott); 146(6): 342–352.
- Safitrih L, Perwitasari DA, Ndoen N, Dandan KL (2019) Health Workers' Perceptions and Expectations of the Role of the Pharmacist in Emergency Units: A Qualitative Study in Kupang, Indonesia. Pharmacy (Basel); 7(1):31.
- Chevalier B, Neville HL, Thompson K, Nodwell L, MacNeil M (2016) Health Care Professionals' Opinions and Expectations of Clinical Pharmacy Services on a Surgical Ward. Can J Hosp Pharm; 69(6): 439–448.
- Schneider PJ (2013) Evaluating the impact of telepharmacy. Am J Health Syst Pharm; 70 (23): 2130-2135.
- Watanabe JH, McInnis T, Hirsch JD (2018) Cost of Prescription Drug-Related Morbidity and Mortality. Ann Pharmacother; 52(9): 829-837.
- Littauer SL, Dixon DL, Mishra VK, Sisson EM, Salgado TM (2017) Pharmacists providing care in the outpatient setting through telemedicine models: a narrative review. Pharm Pract (Granada); 15(4):1134.
- Langarizadeh M, Tabatabaei MS, Tavakol K, Naghipour M, Rostami A, Moghbeli F (2017) Telemental Health Care, an Effective Alternative to Conventional Mental Care: a Systematic Review. Acta Inform Med; 25(4): 240–246.
- Zheng SQ, Yang L, Zhou PX, Li HB, Liu F, Zhao RS (2020) Recommendations and guidance for providing pharmaceutical care services during COVID-19 pandemic: A China perspective. Res Social Adm Pharm;
- Carico RR Jr, Sheppard J, Thomas CB (2020) Community pharmacists and communication in the time of COVID-19: Applying the health belief model. Res Social Adm Pharm; S1551- 7411(20)30293-X.
- Cadogan CA, Hughes CM (2020) On the frontline against COVID-19: Community pharmacists' contribution during a public health crisis. Res Social Adm Pharm. pii:S1551- 7411(20)30292-8.
- Miller S, Patel N, Vadala T, Abrons J, Cerulli J (2012) Defining the pharmacist role in the pandemic outbreak of novel H1N1 influenza. J Am Pharm Assoc (2003); 52 (6): 763-7.
- Sorwar G, Rahamn MM, Uddin R, Hoque MR (2016) Cost and Time Effectiveness Analysis of a Telemedicine Service in Bangladesh. Stud Health Technol Inform; 231: 127-134.
- Vassallo DJ, Swinfen P, Swinfen R, Wootton R (2001) Experience with a low-cost telemedicine system in three developing countries. J Telemed Telecare; 7 Suppl 1: 56-8.
- Rahman MS, Shuvo MH (2015) In J of Innovative Res in Sci, Eng and Tech (IJIRSET); 4 (6): 4810-4822.
- Nessa A, Ameen MA, Ullah S, Kwak KS (2008) Applicability of Telemedicine in Bangladesh: Current Status and Future Prospects. 2008 Third International Conference on Convergence and Hybrid Information Technology: 138-145.
- Khatun F, Heywood AE, Hanifi SMA, Rahman MS, Ray PK, Liaw ST, Bhuiya A (2017) Gender differentials in readiness and use of mHealth services in a rural area of Bangladesh. BMC Health Serv Res; 17(1): 573.
- Ahmed T, Lucas H, Khan AS, Islam R, Bhuiya A, Iqbal M (2014) eHealth and mHealth initiatives in Bangladesh: a scoping study. BMC Health Serv Res; 14:260.
- Hossain MN, Okajima H, Kitaoka H, Yokota F, Ahmed A (2018) eHealth Consumer Behavior. International Series on Computer Entertainment and Media Technology Behavior Engineering and Applications: 129-147.
- Star Online Report. For emergency, dial 999. The Daily Star, December 12, 2017.
- Alif A. Coronavirus: Frustration rising over inadequate hotline services. DhakaTribune, March 19, 2020.
- Baldoni S, Amenta F, Ricci G. (2019) Telepharmacy Services: Present Status and Future Perspectives: A Review. Medicina (Kaunas); 55 (7): 327.
- Poudel A, Nissen LM (2016) Telepharmacy: a pharmacist's perspective on the clinical benefits and challenges [published correction appears in Integr Pharm Res Pract. 2016 Nov 10;5:83]. Integr Pharm Res Pract; 5:75–82.
- Mohiuddin AK (2019) Clinical Pharmacists in Chronic Care. Global Journal of Medical Research: 1-60.
- Alexander E, Butler CD, Darr A, Jenkins MT, Long RD, Shipman CJ, Stratton TP (2017) ASHP Statement on Telepharmacy. Am J Health Syst Pharm; 74 (9): e236-e241.
- Raposo VL (2016) Telemedicine: The legal framework (or the lack of it) in Europe. GMS Health Technol Assess;12: Doc03.
- Crico C, Renzi C, Graf N et al (2018) . mHealth and telemedicine apps: in search of a common regulation. Ecancermedicalscience; 12: 853.
- Cimperman M, Brenčič MM, Trkman P, Stanonik Mde L (2013) Older adults' perceptions of home telehealth services. Telemed J E Health; 19 (10): 786–790.
- van Houwelingen CT, Ettema RG, Antonietti MG, Kort HS (2018) Understanding Older People's Readiness for Receiving Telehealth: Mixed-Method Study. J Med Internet Res; 20(4): e123.
- Jarrett Evans, Amy Papadopoulos, Christine Tsien Silvers, Neil Charness, Walter R. Boot, et al. (2016) Remote Health Monitoring for Older Adults and Those with Heart Failure: Adherence and System Usability. Telemed J E Health 22(6): 480-488.
- Goodridge D, Marciniuk D (2016) Rural and remote care: Overcoming the challenges of distance. Chron Respir Dis 13(2): 192-203.
- Whitten P, Holtz B, Laplante C (2010) Telemedicine: What have we learned? Appl Clin Inform 1(2): 132-141.
- Iftikhar S, Saqib A, Sarwar MR, Sarfraz M, Arafat M, et al. (2019) Capacity and willingness to use information technology for managing chronic diseases among patients: A cross- sectional study in Lahore, Pakistan. Plos One 14(1).
- Zhou L, Thieret R, Watzlaf V, Dealmeida D, Parmanto B (2019) A Telehealth Privacy and Security Self-Assessment Questionnaire for Telehealth Providers: Development and Validation. Int J Telerehabil 11(1): 3-14.
- Smith KA, Zhou L, Watzlaf VJM (2017) User Authentication in Smartphones for Telehealth. Int J Telerehabil 9(2): 3-12.
- Hale TM, Kvedar JC (2014) Privacy and Security Concerns in Telehealth. AMA Journal of Ethics; 16(12): 981-985.
- Arora S, Yttri J, Nilse W (2014) Privacy and Security in Mobile Health (mHealth) Research. Alcohol Res 36(1): 143-151.
- Sankaranarayanan J, Murante LJ, Moffett LM (2014) A retrospective evaluation of remote pharmacist interventions in a telepharmacy service model using a conceptual framework. Telemed J E Health 20 (10): 893-901.
- Nittari G, Khuman R, Baldoni S, Pallotta G, Battineni G, et al. (2020) Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed J E Health.
- Koumaditis K, Themistocleous M, Morabito V (2013) New Trends in Healthcare Information Systems (HIS) Integration. Handbook of Research on ICTs for Human-Centered Healthcare and Social Care Services: 784-801.
- Steckler T (2016) Telepharmacy: Controversy and Promise. J Pharm Technol 32(6): 227-229.
- Marcoux RM, Vogenberg FR (2016) Telehealth: Applications From a Legal and Regulatory Perspective 41(9): 567-570.
- Bashshur RL, Shannon G, Krupinski EA, Grigsby J (2013) Sustaining and realizing the promise of telemedicine. Telemed J E Health 19(5): 339-345.
- Zhao M, Hamadi H, Haley DR, Xu J, White- Williams C, et al. (2020) Telehealth: Advances in Alternative Payment Models. Telemedicine and e-Health.
- Gilman M, Stensland J (2013) Telehealth and Medicare: payment policy, current use, and prospects for growth. Medicare Medicaid Res Rev 3(4): mmrr.003.04.a04.
- Osterweil D (2009) Telehealth Is Ready, Payment System Isnt. Caring for the Ages 10(11): 17.