


Ismail Sezikli1, Ramazan Topcu2*, M. Arif Yuksek3, Orhan Aslan4, M.Oğuzhan Polat5
1Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid: 0000-0002-6801-1465
2Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid: 0000-0001-6214-4868
3Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid: 0000-0002-8323-7390
4Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid: 0000-0002-1982-0792
5Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid: 0009-0004-4725-7425
*Corresponding Author: Ramazan Topcu, Hitit University Faculty of Medicine, Department of General Surgery, 19030, Çorum, Turkey. Orcid No:0000-0001-6214-4868.
Abstract
Background: Laparoscopic cholecystectomy (LC) is a common procedure for gallstones but can lead to complications such as gallbladder perforation and stone spillage. Rarely, gallstones can herniate into unusual locations.
Case Presentation: A 73-year-old male underwent LC and later presented with groin pain. Imaging revealed scattered gallstones within the inguinal canal. Surgical exploration confirmed the presence of gallstones, which were removed, and hernia repair was performed.
Discussion: LC complications can include gallstone spillage, with rare cases leading to extrabiliary complications like inguinal herniation of gallstones. Awareness of such complications is crucial for prompt management.
Conclusion: Clinicians should be vigilant for rare complications post-LC, like gallstone migration into unusual locations, to ensure timely diagnosis and management, thereby improving patient outcomes. Further research is warranted to optimize diagnostic and treatment strategies for these occurrences.
Keywords: Laparoscopic Cholecystectomy, Inguinal Hernia, Scattered Gallstones
Introductıon
Laparoscopic cholecystectomy (LC) is the preferred method for surgically treating symptomatic gallstones due to its advantages of less pain, early mobilization, and improved cosmetic outcomes. Iatrogenic gallbladder perforation and gallstone spillage during LC are common, reported in up to 40% of cases [1,2,3].
Most spilled gallstones are clinically silent and rarely become symptomatic. However, gallbladder hernias containing stones have been reported, albeit rarely [4,5]. Complications can arise from the immediate postoperative period up to 20 years later.
Here, we present a case of scattered gallstones seen in the indirect inguinal hernia sac after LC, along with a literature review.
Case Report
A 73-year-old male patient presented to the General Surgery Clinic 1.5 years ago with symptomatic cholelithiasis and underwent laparoscopic cholecystectomy. Apart from gallbladder perforation with bile and a few gallstones spilling into the peritoneum, there were no specific intraoperative findings. Most stones were removed during surgery. The patient had no complications during follow-up and was discharged on postoperative day 3 in good general condition.
Approximately 14 months after Laparoscopic Cholecystectomy, the patient returned to the clinic with complaints of pain in both groins. Upon examination, a firm mass-like lesion was palpated in the right hernia sac. A computed tomography (CT) scan was ordered, which revealed a diagnosis of bilateral inguinal hernia, with a foreign body measuring approximately 1x1 cm found within the right inguinal canal (Figure 1). Due to the significant pain experienced by the patient, surgical intervention was performed.
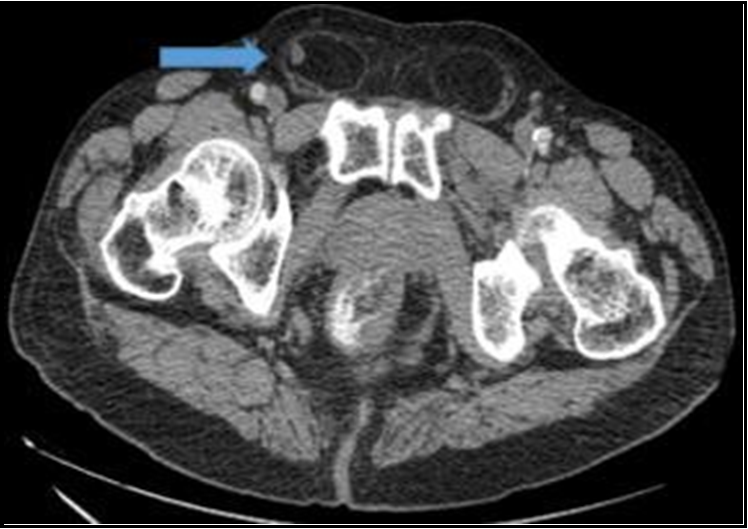
Figure 1: Foreign body in the inguinal canal on CT scan

Figure 2: Intraoperative appearance of gallstones
During surgical exploration on the right side, a foreign body measuring 1x1 cm was observed within the hernia sac (Figure 2). Upon closer examination, it was found that these foreign bodies were consistent with gallstones macroscopically. The gallstone was removed, and bilateral herniotomy and Lichtenstein's prolene mesh repair were performed. The hernia sac and foreign bodies were sent to pathology. The foreign body sent for pathology was reported to be a gallstone measuring 1x0.7x0.5 cm in size, with a yellow-brown color.
Discussion
Although Laparoscopic Cholecystectomy (LC) is preferred for reducing complications and allowing patients to return to their daily lives earlier, it is not without risks. Iatrogenic gallbladder perforation and gallstone spillage are common complications of LC, occurring in up to 40% of cases [1,2,3]. Operative risk factors for iatrogenic gallbladder perforation include surgeon inexperience, difficulty in dissection in the presence of acute cholecystitis, palpation of the gallbladder preoperatively, pain lasting >96 hours preoperatively, and right upper quadrant adhesions from previous abdominal surgeries [6]. Patient characteristics that increase the risk of gallbladder perforation include advanced age, male gender, obesity, and steroid use.
The frequency of early and late complications of gallstone loss is relatively low. Complications can arise from the immediate postoperative period up to 20 years later. Therefore, a patient being discharged with recovery does not necessarily mean that complications will not develop in the future. Common complications of gallstone loss include intraabdominal abscesses with or without a fistulous tract to the abdominal wall, bilio-cutaneous fistula, peritoneal microabscesses and granulomas, liver abscess, retroperitoneal abscess, and rarely thoracic complications [2]. The occurrence of gallstones in the paraumbilical incisional hernia sac, umbilical trocar site hernia sac, and inguinal hernia sac after Laparoscopic Cholecystectomy has been rarely reported [7,8,9].
Shocket reported that stones were left behind in at least 15% of completed laparoscopic cholecystectomies [10]. Almost all of them have been proven to be clinically harmless [10]. Trends have changed, and many authors agree that the removal of all stones after spillage during laparoscopic cholecystectomy is the most appropriate treatment [11,12]. Indeed, some consider stone loss to be an indication for conversion to open cholecystectomy because retained stones can lead to infection [13,14].
This case report concerns the complication of gallstones spreading into the inguinal canal after laparoscopic cholecystectomy. Similar rare cases are limited in the literature, and the management of such cases remains uncertain in many aspects. The spread of gallstones into the inguinal canal is an unexpected complication after surgical intervention, and the mechanism of this condition is not fully understood. Symptoms caused by this condition generally prompt the patient to seek medical attention due to pain and discomfort requiring surgical intervention, as seen in this case presentation. This case underscores the importance of raising awareness of rare complications post-surgery and improving clinical practice in managing similar situations. More case reports on the extrabiliary localization of gallstones should be shared in the literature, and the knowledge and preparedness of the surgical team should be enhanced when encountering such complications. Furthermore, better diagnostic and treatment strategies need to be developed to cope with such rare complications.
In conclusion, rare complications such as the spread of gallstones into the inguinal canal should be considered in the postoperative period. Early diagnosis and effective management are essential to reduce patients' morbidity and mortality risks. Therefore, it is important for the surgical team to be prepared for such rare complications and to determine appropriate treatment strategies.
Ethıcal Declaratıons
Informed Consent: The patient signed the free and informed consent form.
Referee Evaluation Process: Externally peer-reviewed. Conflict of Interest Statement: The authors have no conflicts of interest to declare.
Financial Disclosure: A conflict of interest has not been declared by the author.
Author Contributions: All of the authors declare that they have all participated in the design, execution, and analysis of the paper, and that they have approved the final version.
References
- Sathesh-Kumar T, Saklani AP, Vinayagam R, Blackett RL (2004) Spilled gall stones during laparoscopic cholecystectomy: a review of the literature. Postgrad Med J. 80(940): 77-79.
- Jabbari Nooghabi A, Hassanpour M, Jangjoo A (2016) Consequences of lost gallstones during laparoscopic cholecystectomy: a review article. Surg. Laparosc. Endosc. Percutan. Tech. 26(3): 183–192.
- Trerotola SO, Lillemoe KD, Malloy PC, Osterman FA (1993) Percutaneous removal of “dropped” gallstones after laparoscopic cholecystectomy. Radiology. 188(2): 419–421.
- Bebawi M, Wassef S, Ramcharan A, Bapat K (2000) Incarcerated indirect inguinal hernia: a complication of spilled gallstones. JSLS. 4(3): 267-269.
- Bolat H, Teke Z (2020) Spilled gallstones found incidentally in a direct inguinal hernia sac: Report of a case. Int J Surg Case Rep. 66: 218-220.
- Assaff Y, Matter I, Sabo E, Mogilner JG, Nash E, et al. (1998) Laparoscopic cholecystectomy for acute cholecystitis and the consequences of gallbladder perforation, bile spillage, and "loss" of stones. Eur J Surg. 164(6): 425-31.
- Rosin D, Korianski Y, Yudich A, Ayalon A (1995) Lost gallstones found in a hernial sac. J. Laparoendosc. Surg. 5(6): 409–411.
- Aspelund G, Halldorsdottir AB, Isaksson HJ, Moller PH (1999) Case of the month. Gallstone in hernial sack. Laeknabladid. 85: 218–219.
- Demirbas BT, Gulluoglu BM, Aktan AO (2015) Retained abdominal gallstones after laparoscopic cholecystectomy: a systematic review. Surg Laparosc Endosc Percutan. Tech. 25(2): 97–99.
- Shocket E (1995) Abdominal abscess from gallstones spilled at laparoscopic cholecystectomy. Surg Endosc. 9(3): 344–347.
- Leslie KA, Rankin RN, Duff JH (1994) Lost gallstones during laparoscopic cholecystectomy; are they really benign? Can J Surg. 37: 240–242.
- Strasberg SM, Sanabria JR, Clavien PA (1992) Complications of laparoscopic cholecystectomy. Can J Surg. 35(3): 275-280.
- Deziel DJ, Millikan KW, Economou SG, Doolas A, Ko ST, et al. (1993) Complications of laparoscopic cholecystectomy: a national survey of 4,292 hospitals and an analysis of 77,604 cases. Am J Surg. 165(1): 9–14.
- Wilton PB, Andy OJ Jr, Peters JJ, Thomas CF, Patel VS, et al. (1993) Laparoscopic cholecystectomy. Leave no spilled stone unturned. Surg Endosc. 7(6): 537–538.