


Vamsidhar Veeranki1, Anupma Kaul4*, Jeyakumar Meyyappan1, Durgesh kumar Pushkar1, Narayan Prasad4, Dharmendra Bhadauria3, Manas Ranjan Behera2, Monika Yaccha2, Ravi Shankar Kushwaha2, Prabhakar Mishra5, Vinita Aggrawal6
1Assistant Professor MD; DM Department of Nephrology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
2Associate Professor MD; DM Department of Nephrology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
3Additional Professor MD; DM Department of Nephrology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
4Professor MD; DM Department of Nephrology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
5Associate Professor, Department of Biostatistics, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
6Professor, Department of Pathology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow
*Corresponding Author: Anupma Kaul, Professor MD; DM Department of Nephrology and Renal Transplantation, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow.
Abstract
Background
Patients with end-stage renal disease (ESRD) were found to be at an increased risk of psychological stress, which got further worsened with COVID-19. We assessed the psychosocial stressors among the patients on maintenance hemodialysis (MHD) who developed COVID-19.
Methods
This prospective study was conducted on patients with CKD who were on MHD and infected with SARS-CoV2 during the first or second Indian pandemic waves. The primary objective is to study the change in Kessler-6 score during the SARS-CoV2 infection. The secondary objectives include analysis of the factors associated with the increased stress and to explore the significant stressors among this cohort.
Results
The K-6 scores during the SARS-CoV2 infection were found to be significantly higher (10.8>0.9) in comparison with the K6 scores before illness (6.6±1.5), with a mean increase of 4.2±0.5 (p = 0.02). Age > 40 years, dialysis duration < 3 years, rural residency, and rented transport facilities were associated with increased psychosocial stress (K-6 score13) on Cox multivariate analysis. The major stressor for the COVID effect was the accessibility to the MHD center (59 %). The stress regarding the COVID-19 disease was seen only in 13 % of the COVID-affected patients.
Conclusions
Patients on MHD tend to have increased stress levels when affected by COVID-19, with the significant stressor being the accessibility to a dialysis facility. Hence, reforms in the health care system to improve the accessibility to dialysis are needed to improve the mental health and thus, overall survival of dialysis-dependent patients.
Introduction
Patients with end-stage renal disease (ESRD) were found to be at an increased risk of psychological stress due to their underlying chronic illness and the added stress of thrice-weekly maintenance hemodialysis [1,2]. Various observational studies have shown that about 6 -8 % of the patients on maintenance dialysis have major depression, and at least 16 – 20 % have been suffering from minor depression [3,4]. These psychiatric issues were further worsened by COVID-19, the biggest disaster of this decade, which increased stress and anxiety levels even in the general population [5-7]. More than 25 % of CKD patients on maintenance hemodialysis (MHD) were found to have psychiatric issues during the COVID pandemic. Besides the 2.5 times increased risk of mortality due to COVID-19 in the MHD population, they are also at an increased risk of mental stress due to the disease [5]. The increased psychological stress for this vulnerable cohort during the COVID-19 pandemic is multifactorial – 1. Impact of lockdown on their acquisition of thrice-weekly maintenance hemodialysis without which their life will be endangered [8] 2. The potential risk of acquiring SARS-CoV2 infection while traveling to or at the dialysis center 3. The financial burden imposed by the pandemic situation and lockdown 4. Limited centers provide dialysis facilities, as most are converted to COVID-care facilities [9,10]. This ultimately led to a deficit in dialysis facilities and increased mortality among many dialysis-dependent patients [11].
Besides these psychosocial stressors among dialysis patients due to the pandemic around, mental stress worsens once they acquire COVID-19 because of the following reasons – 1. Impact of grave outcomes of COVID-19 as they see and hear around them, 2. Limited availability of COVID-19 dedicated day-care dialysis facilities, 3. Mandatory hospitalization (at many centers during the first wave) for getting dialyzed despite being asymptomatic, 4. Limited availability of beds in COVID-19 dedicated centers 5. The stress of isolation added to the background stress of the chronic disease [12]. Many studies have looked into its impact on the non-dialysis-dependent CKD population with mixed results, some showing no significant increase in the levels of distress [13] while others revealing an alarming psychological effect [6,14]. These studies focused on the impact of the COVID-19 pandemic on the CKD population (non- dialysis dependent and dependent), but no studies have focused on those directly affected by COVID-19. The apprehensions due to COVID-19 among those with underlying chronic illness and, above all, among the dialysis population seem unexplored. Besides the standard medical care these patients require, it is also essential to evaluate the psychological impact of the current pandemic and try to alleviate them. Hence, the present study aimed to assess the psychosocial stressors and the difficulties faced by ESRD patients who developed COVID-19 and devise strategies to ease the stresses during further waves of the COVID-19 pandemic or similar disasters.
Objectives:
Primary Objective:
To study the change in Kessler-6 score during the SARS-CoV2 infection from that of baseline score before infection among the patients on maintenance hemodialysis.
Secondary Objectives:
1. To compare characteristics of patients who had increased levels of stress (K-6 score 13) to those who had no increased levels of stress while infected with SARS-CoV2.
2. To study the factors associated with increased stress during COVID-19 among the ESRD population.
3. To study the significant stressors during COVID-19 in the ESRD population.
4. To study various methods the ESRD population adopts to combat stress during COVID-19.
5. To assess the psychological support received by the ESRD population during COVID-19 from a patient's perspective.
Materials and Methods
Study design and setting
This is a prospective study conducted on patients with chronic kidney disease (CKD) who were on maintenance hemodialysis in our institute (SGPGIMS, Lucknow) and infected with SARS-CoV2 either during the first Indian pandemic wave (25th March 2020 to 31st January 2021) or the second Indian pandemic wave (1st March 2021 to 31st July 2021). CKD patients not on dialysis and patients on peritoneal dialysis were excluded. The psychological status of these patients was assessed using the K-6 questionnaire. The Kessler-6 scale is a 6-item self-report measure of psychological distress intended to be used as a quick tool to determine the risk for severe mental illness in the general population [15]. It is a validated tool for assessing mental health in patients with CKD or COVID-19 [16-18]. As shown in Figure 1., it analyses psychosocial stress by determining the mental condition over the past 4 weeks across 6 domains with a 5-point ordinal score of 0 – 4, 0 being "none of the time" and 4 beings "all of the time." With a maximum score of 24, patients were categorized into 3 categories of distress based on the K6 scores: none (scores of 0-7), mild to moderate (scores of 8-12), and severe (scores of 13-24), the latter of which is associated with a high probability of having a debilitating mental illness.
K6 scores of ESRD patients were calculated by direct questionnaire at baseline before the SARS-CoV2 infection and when they were infected with SARS-CoV2. Rajdhani COVID Hospital (RCH), our center's dedicated COVID-19 care facility, has both in-patient and outpatient dialysis facilities. ESRD patients with COVID-19 are dialyzed on an in-patient or outpatient basis depending on the patient's choice, the severity of the COVID, and other logistics such as availability of transport facilities, care providers, etc. Patients under asymptomatic, mild, and moderate severity categories at admission were included in the study. The K6 scores during the SARS-CoV2 infection were assessed within 1 week of diagnosis of COVID either during the hospitalization or when they were being dialyzed in the COVID-dedicated dialysis unit in our center. Patients were also asked about various events leading to psychological stress before and during infection. Apart from the patients' socioeconomic, demographic, and educational status, the questionnaire regarding changes in the lifestyle they had adopted to combat the stress and the central psychological support was also included (Figure 1).
|
During the past 4 weeks (28 days), how much of the time did u feel? |
|||||
|
|
None of the time (0) |
A little of the time (1) |
Some of the time (2) |
Most of the time (3) |
All of the time (4) |
|
…So sad nothing could cheer you up? |
|
|
|
|
|
|
…nervous? |
|
|
|
|
|
|
…restless or fidgedity? |
|
|
|
|
|
|
…hopeless? |
|
|
|
|
|
|
…that everything was an effort? |
|
|
|
|
|
|
…worthless? |
|
|
|
|
|
|
Summary of the questionnaire to assess the psychological stress in the study population
|
|||||
Figure 1: K-6 questionnaire and the summary of questions asked to assess the psychological stress in ESRD patients
Statistical analysis
All the continuous data were expressed in mean or median depending on the normality of the data. The mean change in K-6 scores before and after SARS-CoV2 infection was compared with the paired t-test. Categorical data were expressed in proportions/ ratios. Student's t-test/Mann-Whitney's U-test was used to compare quantitative data based on normality. Qualitative data were analyzed by Chi-square test. All the significant (p<0.05) and marginal important (p < 0.1) variables in univariate analysis were included in multivariate binary logistic regression analysis to identify the independent predictors of the stressed patients (K 13). Assuming 50 % of dialysis patients during COVID-19 were under some stress, at minimum two-sided 95% confidence interval and 12.5 % margin of error in supposed prevalence, the estimated sample size is 62. The sample size was calculated using software Power analysis and sample size version 16. Statistical package for social sciences, version -23, and Med Calc, version 20, to be used for data analysis.
Results
Baseline characteristics
68 patients on maintenance dialysis who developed COVID during the first or second pandemic waves were included for analysis. The baseline characteristics are shown in Table 1. The mean age of the study population was 35.4±6.8 years, and 58.8 % were males. The mean duration of dialysis before SARS-CoV2 infection was 3.7±2.8 years. The associated chronic co-morbid conditions included hypertension in 58 (85.2 %), hypothyroidism in 6 (8.8 %), post-transplant graft failure in 6 (8.8 %), and diabetes mellitus in 3 (4.4 %). In the study population, the literacy rate as defined by the Indian Government was 95.6 %, well above the national average of 74.04 % [19]. Of them, 11.7 % had primary education, 47.1 % had secondary education, and 36.7 % had higher education, including graduation. The socioeconomic assessment done by the Kuppuswamy scale revealed that most of the patients (57.3 %) belong to the lower-middle-class group (Class III). In the study population, 73.6 % reside in an urban locality, while 26.4 % reside in rural areas. Even before the pandemic, 45.6 % felt that access to healthcare was difficult. While 45.6 % of patients had their private vehicle for dialysis, 33.8 % used a rented transport service, and 20.6 % used to come on foot to the MHD center.
Table 1: Baseline characteristics of ESRD patients undergoing maintenance hemodialysis
|
Variable |
N = 68 |
|
Age (years, Mean± SD) |
35.4±6.8 |
|
Gender, N (%) Males Females |
40 (58.8 %) 28 (41.2 %) |
|
Mean duration of dialysis prior to COVID-19 pandemic, years, Mean± SD (Range) |
3.7±2.8 (1.1 – 7.4) |
|
Severity of COVID Asymptomatic Mild Moderate |
11 (16.1 %) 44 (64.7 %) 13 (19.1 %) |
|
Time since initiation of hemodialysis, N (%) < 3 years 3-5 years > 5 years |
15 (22 %) 34 (50 %) 19 (28 %) |
|
Post-transplant-ESRD (CKD-5TD), N (%) |
6 (8.8 %) |
|
Other Comorbidities, N (%) Hypertension Hypothyroidism Diabetes Mellitus Bronchial asthma/COPD CAD Seizures No other comorbidities |
58 (85.2 %) 6 (8.8 %) 3 (4.4 %) 3 (4.4 %) 2 (2.9 %) 2 (2.9 %) 6 (8.8 %) |
|
Literacy status, N (%) Higher education Secondary education Primary education Illiterate |
25 (36.7 %) 32 (47.1 %) 8 (11.7 %) 3 (4.4 %) |
|
Modified Kuppuswamy SES scale* I. Upper (26 – 29) II. Upper middle class (16 – 25) III. Lower middle class (11 – 15) IV. Upper Lower class (5 -10) V. Lower class (<5) |
1 15 (22 %) 39 (57.3 %) 13 (19.1 %) 0 |
|
Residency, N (%) Urban Rural |
50 (73.6 %) 18 (26.4 %) |
|
Ease of health care access, N (%) Easy (< 10 km) Difficult (> 10 km) |
37 (54.4 %) 31 (45.6 %) |
|
Travel from home to dialysis centre, N (%) By private vehicle By public access On foot |
31 (45.6 %) 23 (33.8 %) 14 (20.6 %) |
ESRD: End stage renal disease; COPD: Chronic obstructive pulmonary disease; CAD: Coronary artery disease; SES: Socioeconomic scale;
Outcome analysis:
1. Primary Outcome
As shown in Figure 1, the K-6 scores during the SARS-CoV2 infection were found to be significantly higher (10.8>0.9) in comparison with the K6 scores before infection (6.6±1.5) with a mean increase of 4.2±0.5 (p = 0.02). A total of 15 patients (22 %) had a K6 score ≥13 while infected with SARS-CoV2.
2. Secondary outcome
A) Factors associated with increased stress during the COVID-19 among the ESRD population:
As shown in Table 2., the baseline characteristics of patients with a K-6 score of 12 were compared to those with a K-6 score ≥13. The mean age was significantly higher in the latter group (48.5 vs. 31.6 years, p < 0.001), while they were on substantially shorter duration of dialysis (28.4 vs. 44.7 months, p < 0.001).
Among patients who reported higher psychosocial stress (K613), most of them belonged to rural areas (73.3 % Vs. 26.6 %, p < 0.001); and many had difficult access to dialysis centers (73.3 % vs. 37.8 %, p = 0.01); used public transport system for conveyance (66.6 % vs. 24.5 %, p = 0.002). On performing a Cox multivariate analysis (Table 3), age > 40 years, dialysis duration of < 3 years, rural residency, and the use of rented transport facility were the factors associated with increased psychosocial stress ( K-6 score13)
Table 2: Comparison of baseline characteristics between patients with and without K6 scores ≥13.
|
Variable |
K6 < 12 (n = 53) |
K6 > 13 (n = 15) |
p-value |
|
Mean age |
31.6±8.2 |
48.5±3.2 |
< 0.001 |
|
Gender (Male, %) |
32 (60.3 %) |
8 (53.3 %) |
0.62 |
|
Severity of COVID Asymptomatic Mild Moderate |
8 (15.1 %) 36 (67.9 %) 9 (16.9 %) |
3 (25 %) 8 (53.3 %) 4 (26.6 %) |
0.37 0.29 0.4 |
|
Mean duration of dialysis |
44.7±8.7 |
28.4±4.7 |
< 0.001 |
|
Post-transplant-ESRD (CKD-5TD), N (%) |
4 (7.5 %) |
2 (13.3 %) |
0.4 |
|
Other Comorbidities, N (%) Hypertension Hypothyroidism Diabetes Mellitus Other comorbidities No other comorbidities |
47 (88.6 %) 4 (7.5 %) 3 (5.6 %) 2 (3.6 %) 5 (9.4 %) |
11 (73.3 %) 2 (13.3 %) 0 5 (33.3 %) 1 (6.6 %) |
0.14 0.48 0.35 < 0.001 0.73 |
|
Literacy status, N (%) Secondary education and above Primary Education Illiterate |
49 (92.5 %) 3 (5.6 %) 1 (1.9 %) |
8 (53.3 %) 5 (33.3 %) 2 (13.3 %) |
< 0.001 0.003 0.06 |
|
Modified Kuppuswamy SES scale* I. Upper (26 – 29) II. Upper middle class (16 – 25) III. Lower middle class (11 – 15) IV. Upper Lower class (5 -10) V. Lower class (<5) |
1 (1.8 %) 11 (20.7 %) 31 (58.4 %) 10 (18.8 %) 0 |
0 4 (26.6 %) 8 (53.3 %) 3 (20 %) 0 |
0.6 0.62 0.73 0.92 0 |
|
Residency, N (%) Urban Rural |
46 (86.7 %) 7 (13.2 %) |
4 (26.6 %) 11 (73.3 %) |
< 0.001 |
|
Ease of access to a dialysis center, N (%) Easy (< 10 km) Difficult (> 10 km) |
33 (62.2 %) 20 (37.8 %) |
4 (26.6 %) 11 (73.3 %) |
0.01 |
|
Travel from home to dialysis centre, N (%) By private vehicle By rented transport facility On foot |
28 (52.8 %) 13 (24.5 %) 12 (22.6 %) |
3 (20 %) 10 (66.6%) 2 (13.3 %) |
0.02 0.002 0.4 |
*Analysed as per the Kuppuswamy socio-economic status scale 2021 [21]
ESRD: End stage renal disease; COPD: Chronic obstructive pulmonary disease; CAD: Coronary artery disease; SES: Socioeconomic scale;
Table 3: Factors associated with increased stress (K6 score ≥13) in ESRD population during COVID-19 (By Cox Univariate and multivariate regression analysis)
|
Variable |
Odds ratio (95% CI) |
p-value |
|
Univariate analysis |
||
|
Age group (> 40 years) |
68.3 (4.7 – 766.2) |
< 0.001 |
|
Duration of dialysis |
28.6 (5.97 – 128.3) |
0.01 |
|
Education (< Secondary education) |
19.52 (13.2 – 139.9) |
<0.001 |
|
Ease of access to a dialysis center |
30.26 (22.8 – 155.7) |
0.01 |
|
Rural residence |
37.3 (22.9 – 162.7) |
< 0.001 |
|
Rented transport facility |
48.7 (5.82 – 213.7) |
0.002 |
|
Multivariate analysis* |
||
|
Age group (> 40 years) |
50.5 (5.25 – 485.9) |
< 0.001 |
|
Dialysis Duration < 3 years |
12.8 (4.82 – 96.26) |
0.04 |
|
Rural Residence |
18.98 (3.02 – 119.49) |
0.02 |
|
Rented Transport facility |
20.11 (2.93 – 138.3) |
0.02 |
*Factors significant in univariate analysis are taken for analysis in multivariate analysis
B) Stressors during COVID in the ESRD population:
As shown in Figure 3, the major stressors for the ESRD population when they were affected by COVID was the accessibility to the MHD center (59 %), followed by the stress due to isolation (16 %) or hospitalization (12 %). The stress regarding the COVID-19 disease was seen only in 13% of the COVID-affected patients.
C) Various methods adopted by the ESRD population to combat stress during COVID
(Figure. 4a)
When asked about various measures adopted to combat stress, 63.2 % of the study population replied that spiritual methods were the primary stress relief measure, followed by increased use of social media (58.8 %). 54.5 % of the study population replied that they had spent more time with their family and pandemic had brought them closer to their family. While one patient had increased substance abuse (alcohol intake), 23.5 % could not adapt to the changes in their lifestyle during COVID.
D) The primary support system of COVID affected the MHD population during the pandemic from the patient's perspective
As depicted in Figure 4b, the central support system that the patients received was their trust in God (59 %), followed by support from family and friends (25 % and 10 %, respectively). The health care system support was considered significant in only 6 % of the study population.
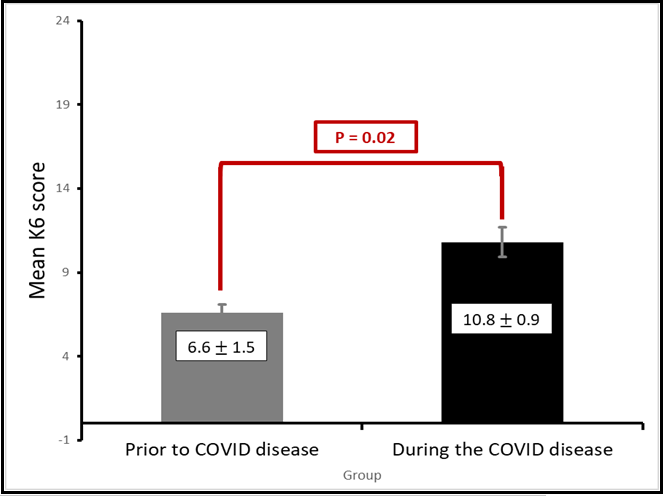
Figure 2: K6 scores pre and post SARS-CoV2 infection in ESRD population during the pandemic
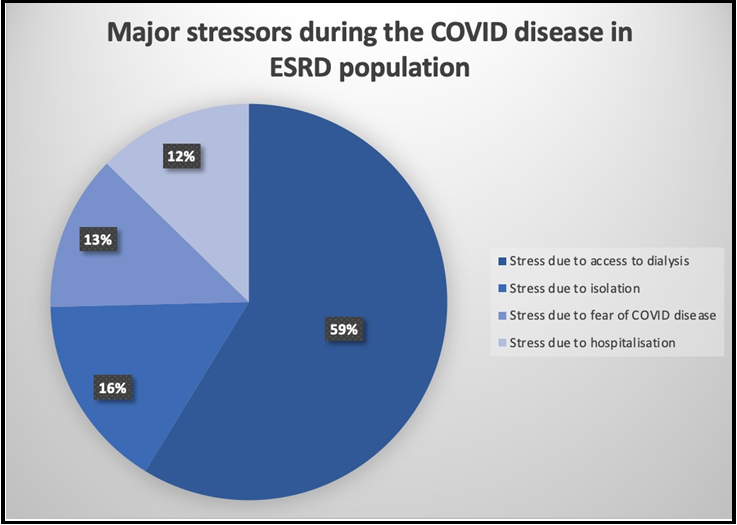
Figure 3: Major stressors in ESRD population while affected with COVID-19
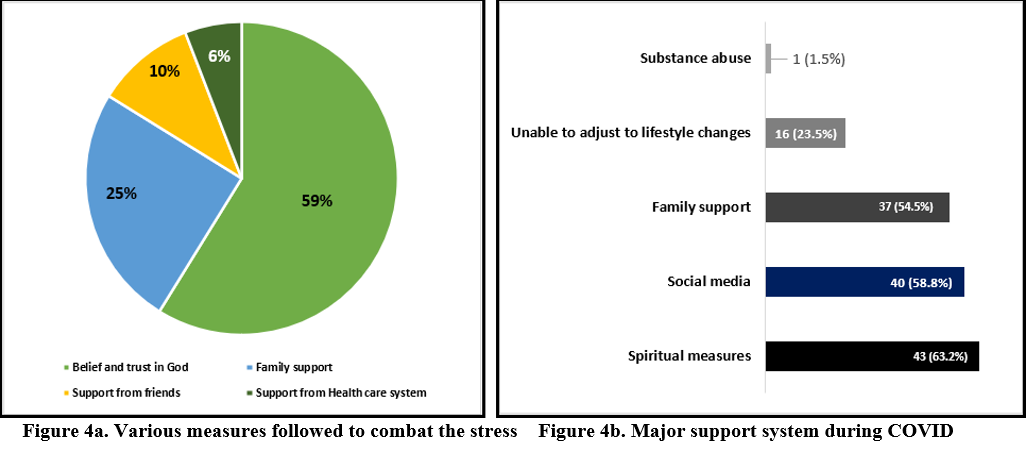
Figure 4: Various ways used by ESRD population to combat the stress while affected with COVID-19 and the major support system from a patient’s perspective
Discussion
The psychological stress in the dialysis-dependent population, more so in the era of COVID-pandemic is understandable yet unexplored. This is the first study on the psychological aspects of COVID affected dialysis population. The study hypothesized that individuals with ESRD have increased levels of psychological distress when affected by COVID-19 compared to the baseline. For this purpose, the baseline psychological stress among the individuals on MHD before SARS- CoV2 infection was compared to when they were affected by COVID-19. K-6 score, a validated tool for assessing the psychological distress in the CKD population [16,18], was used in our study. We observed that the mean K-6 score in the study population significantly increased when they were affected by COVID-19 compared to the baseline. Though both the K-6 scores before and during COVID were less than the severe stress levels (K-6≤12), a significant increase in the mean K-6 score during the COVID disease is bothersome. Similar findings were found in prior studies, where a substantial increase in stress levels was noted in the ESRD patients during the COVID pandemic compared to the pre-pandemic period [13,14]. But prior studies did not analyze the stress levels among the patients affected by COVID-19.
We also observed that > 20 % of the patients had severe levels of psychological distress during COVID-19, with K-6 scores of 13. We found that this subset of the population was on dialysis for a significantly shorter duration of time, was older, and had less educational status compared to those with a score of 12. Many of these patients were found to be residing in rural areas and had to access dialysis centers using public transport services. However, the severity of COVID-19 did not differ between the two groups, which could imply that even during COVID-19, the psychosocial stress in the ESRD population was influenced by socioeconomic background rather than the disease severity. Cox multivariate regression analysis to assess the predictors of stress during the COVID-19 disease revealed that age > 40 years, dialysis duration < 3 years, rural residence, and use of public transport facility for dialysis were associated with severe levels of psychological distress among the COVID-affected ESRD patients. Hence, apart from the older patients, patients with practical difficulties in accessing dialysis facilities were found to have increased stress levels. Also, patients on dialysis for a shorter duration, i.e., "the less-experienced dialysis-dependent" patients, were at an increased risk of psychological distress. A similar finding was also observed in a Chinese study where the shorter duration of dialysis was associated with higher levels of psychological stress during the COVID pandemic [20]. These subgroups with increased stress levels have a common feature of difficulty in accessing the dialysis center. This was re-affirmed when we found that the majority of the individuals (59 %) opined that the significant stressor for them was regarding access to a dialysis center. More importantly, only 13 % of the patients had stress due to COVID disease per se. Hence for an individual with MHD, even after getting affected by an illness that could be life-threatening, the primary concern is regarding the accessibility to the dialysis facility.
Surprisingly, an individual's socioeconomic status had no association with psychological stress in our study. This is in contradiction to what was observed by Choi et al., 2019 [16], in their pioneering study, found that in a given individual, their socioeconomic status and hence the financial accessibility to subspecialty care and dialysis facilities have got a significant influence on the degree of psychological stress (assessed by K-6 scoring as well). This situation was expected to further worsen during the COVID pandemic. The lack of association with socioeconomic status in our study could be because most patients (nearly 60 %) were from a lower socioeconomic status (Kuppuswamy classification - Class III - Lower middle socioeconomic class).
Analysis of the effective stress-relieving methods to adjust to the lifestyle changes during the COVID revealed that most patients (63 %) followed spiritual procedures for stress relief, followed by social media and family support. Approximately 23.5 % of the patients could not adjust to the lifestyle changes. When asked about the effective support system among COVID-19-affected dialysis patients, most (nearly 60 %) revealed spiritual support, followed by family support (25 %). Unfortunately, only 6 % of the patients felt that the healthcare system was their significant support. This is even though the ESRD cohort is one such patient population in close and frequent contact with the healthcare system. Hence considerable reforms in the health care system to promote psychosocial care and, therefore, the overall survival of dialysis-dependent populations are necessary. The practical measures to improve the dialysis population's care and psychosocial health during a pandemic are summarized in Figures 5a and 5b.
One of the significant limitations of the study is the referral bias. The study was conducted in a tertiary center catering to patients mainly from lower socioeconomic status, so the results might not be extrapolated to other classes. Secondly, the K-6 scoring system predicts the stress levels that the patient had over the last month. But the effect of the background stress might have been partially nullified by using the baseline K-6 score before COVID. Lastly, the results are limited to ESRD patients with asymptomatic/ mild/ moderate categories of COVID. The study's strengths are the prospective design, and the real-time data collection by the direct-interview method, which should avoid recall bias. The complete psychological stress assessment done by a multi-dimensional tool like the Kessler-6 scoring system gives a holistic view of the psychological status of dialysis-dependent patients.
Conclusion
To conclude, we assessed the direct effect of COVID on the mental health of the ESRD population, a neglected cohort, particularly in terms of the psychosocial domain. We found that the ESRD population has an increased baseline psychological stress and tends to have further increased levels of anxiety when they are affected by COVID-19. Patient subgroups with difficult accessibility to dialysis facilities are particularly at an increased risk of stress. The major stressor for most ESRD patients, even while they were affected by COVID, is the accessibility to a dialysis facility. Hence, reforms in the health care system by allocating resources to improve the accessibility to dialysis are needed in the current pandemic to improve the mental health and overall survival of dialysis-dependent patients.
Authorship contribution statement
Anupma Kaul, Vamsidhar Veeranki, Narayan Prasad, and Dharmendra Bhadauria Participated in the research design.
Vamsidhar Veeranki, Anupma Kaul, Jeyakumar Meyyappan participated in the writing of the paper.
Narayan Prasad, Dharmendra Bhadauria, Manas Ranjan Behera, Monika Yachha and Ravi Shankar Kushwaha participated in the performance of the research.
Prabhakar Mishra and Vinita Aggrawal participated in data analysis
Disclosure: The authors declare no conflicts of interest
Funding: No funding
References
- Kimmel PL (2000) Psychosocial factors in adult end-stage renal disease patients treated with hemodialysis: correlates and outcomes. Am J Kidney Dis. 35(4 Suppl 1): S132-40.
- Chan R, Steel Z, Brooks R, Heung T, Erlich J, et al. (2011) Psychosocial risk and protective factors for depression in the dialysis population: a systematic review and meta-regression analysis. J Psychosom Res. 71(5): 300-10.
- Hinrichsen GA, Lieberman JA, Pollack S, Steinberg H (1989) Depression in hemodialysis patients. Psychosomatics. Psychosomatics. 30(3): 284-9.
- Kimmel PL, Thamer M, Richard CM, Ray NF (1998) Psychiatric illness in patients with end-stage renal disease. Am J Med. 105(3): 214-21.
- McGinty EE, Presskreischer R, Han H, Barry CL (2020) Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA. 324(1): 93-94.
- Lee J, Steel J, Roumelioti ME, Erickson S, Myaskovsky L, et al. (2020) Psychosocial Impact of COVID-19 Pandemic on Patients with End-Stage Kidney Disease on Hemodialysis. KIDNEY 360. 1(12): 1390–1397.
- Chan ASW, Ho JMC, Li JSF, Tam HL, Tang PMK (2021) Impacts of COVID-19 Pandemic on Psychological Well-Being of Older Chronic Kidney Disease Patients. Front Med (Lausanne). 8: 666973.
- The Effects of India’s Covid-19 Lockdown on Critical Non-Covid Health Care and Outcomes.
- COVID-19 cost: Dialysis takes a backseat.
- COVID-19 and its Impact on Kidney Patients Utilizing U.S. Dialysis Centers.
- Prasad N, Bhatt M, Agarwal SK, Kohli HS, Gopalakrishnan N, et al. (2020) The Adverse Effect of COVID Pandemic on the Care of Patients With Kidney Diseases in India. Kidney Int Rep. 5(9): 1545-1550.
- Guidelines for Dialysis of COVID – 19 patients.
- Bonenkamp AA, Druiventak TA, van Eck van der Sluijs A, van Ittersum FJ, van Jaarsveld BC, et al. (2021) The Impact of COVID-19 on the mental health of dialysis patients. J Nephrol. 34(2): 337-344.
- Yu JY, Kim JS, Hong CM, Lee KY, Cho NJ, et al. (2021) Psychological distress of patients with end-stage kidney disease undergoing dialysis during the 2019 coronavirus disease pandemic: A cross-sectional study in a University Hospital. PLoS One. 16(12): e0260929.
- Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, et al. (2003) Screening for serious mental illness in the general population. Arch Gen Psychiatry. 60(2): 184-9.
- Choi NG, Sullivan JE, DiNitto DM, Kunik ME (2019) Health Care Utilization Among Adults With CKD and Psychological Distress. Kidney Med. 1(4): 162-170.
- Lyons Z, Wilcox H, Leung L, Dearsley O (2020) COVID-19 and the mental well-being of Australian medical students: impact, concerns and coping strategies used. Australas Psychiatry. 28(6): 649-652.
- Katayama A, Miyatake N, Nishi H, Hashimoto H, Uzike K, et al. (2015) Evaluation of psychological distress using the K6 in patients on chronic hemodialysis. Environ Health Prev Med. 20(2): 102-7.
- Literacy of Rural – Urban. https://censusindia.gov.in/2011-prov- results/paper2-vol2/data_files/AP/Chapter_VI.pdf.Date accessed: February 12, 2022.
- Yang ZH, Pan XT, Chen Y, Wang L, Chen QX, et al. (2021) Psychological Profiles of Chinese Patients With Hemodialysis During the Panic of Coronavirus Disease 2019. Front Psychiatry. 12: 616016.
- Saleem SM, Jan SS (2021) Modified Kuppuswamy socioeconomic scale updated for the year 2021. Indian J Forensic Community Med. 8(1):1-3.