


Mossaab Ghannouchi1*, Matoug Mohamed2, Ben Khlifa Mohamed1, Morthadha Boukhchim1, Nacef Karim1, Boudokhan Moez1
1General surgery department Tahar sfar hospital Mahdia Tunisia
2services A21 charle nicole Tunisia
*Corresponding Author: Ghannouchi Mossaab, General surgery department Tahar sfar hospital Mahdia Tunisia.
Introduction
Post-traumatic hernia (HPT) of the abdominal wall is a rare entity, defined by the protrusion of an organ, or pre-peritoneal fat through an acquired defect of the musculoaponeurotic wall following a trauma, without the notion of pre-existing hernia. [1] The first case was described by Shelby in 1906 and since then around 250 cases have been published [2]. The preferential location of HPTs in the abdominal wall is in areas of weakness [3], the spiegel line of which remains an exceptional location and is rarely reported in the literature. [4] This is how we propose to take stock of this entity in order to emphasize its rarity and diagnostic difficulties since it is often overlooked in emergency situations.
Observation
We report the case of a 27-year-old patient with no pathological history who consulted in the emergency room following a stabbing attack. He was stabbed in his abdomen as a result of a fight. On initial examination, he was hemodynamically stable. Abdominal examination found only a 2 cm linear wound on the left flank with unshredded edges without evisceration or from the digestive fluid. The abdomen was supple without any palpable swelling. Biology showed hyperleukocytosis at 17100. Thoraco-abdominal computed tomography did not show traumatic intra-abdominal lesions apart from a diastasis between the rectus abdominis and the muscles of the left anterolateral wall of the abdomen without intraabdominal effusion. (Figure 1) It was decided to hospitalize and monitor the patient in a surgical setting. Faced with the installation of an abdominal defense at the level of the left half-abdomen, it was decided to operate on the patient via the midline. On exploration, the abdominal wound was non- penetrating, the small intestine was dilated upstream of a loop incarcerated at the level of a left spiegel hernia, which was released with good vitality. (Figure 2) The hernial orifice was closed with Vicryl 1.0 stitches. The post-operative consequences were simple. The exit was authorized after 3 days.

Figure 1: Abdominal CT scan showing a defect of the anterior abdominal wall (arrow)
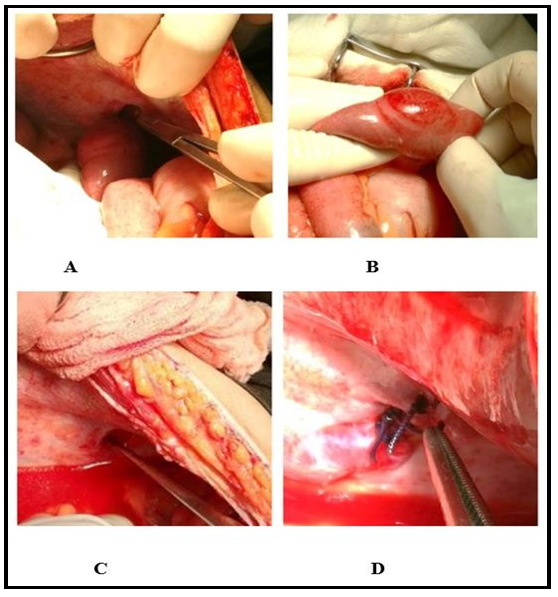
Figure 2: Vue per operatoire A-B: anse incrarceree, C-D: orifice herniaire au niveau de la Ligne de spiegel
Discussion
The first case of post-traumatic spiegel hernia dates back to the year 1933 described by Brandtner [5] and since a few cases have been reported [Table 1]. HPT remains a rare clinical entity with a prevalence of 1 % in all patients. Patients presenting with abdominal trauma [6] It occurred in direct shock after abdominal trauma causing a sudden increase in intra-abdominal pressure. This shock must be spread over a large enough area, without having the force necessary to be penetrating, but still capable of breaking deeper tissues, muscles, and fascia. The hernia is not seen in the site of trauma but in anatomical points of weakness such as the spiegel line [1,7]. This HPT most often occurs after a low energy mechanism (collision between two motorcycles, contusion by bicycle handlebars ...) more rarely during 'high-energy trauma (AVP with deceleration, fall from a high height) which will be associated with a large wall defect and greater intra-abdominal lesions [8].
This post-traumatic parietal lesion may be unrecognized especially when it is small and especially in an emergency context [9]. In a series published by Netto et al. [6] comprising 34 cases of PTH of which 30% are not palpable on clinical examination, 50 % are associated with intra- abdominal lesions requiring urgent laparotomy, for the other patients having non-operative treatment two developed a subsequent hernial constriction with an urgent repair. The rate of hernial strangulation for HPT is 8 to 25 % depending on the series [6] which may appear secondarily as in our case, hence the interest of computed tomography which remains essential for the diagnosis of hernia and looking for an associated intra-abdominal lesion. Surgical treatment is urgent in case of associated lesions or hernial strangulation. If the treatment is deferred, the median or elective approach, by laparotomy or laparoscopy, repair with a suture or a plate are still discussed. However, until now, the authors recommend urgent exploration of any HPT by a midline with suturing of the defect by a nonabsorbable thread [10] but with a rate of recurrence after a herniorrhaphy not yet specified requiring the use of series with longer follow-up. [6]
Table 1: Characteristics of patients with post-traumatic spiegel hernia
|
|
year |
âge |
mechanism |
Clinical examination |
Scanner |
incision |
Exploration+ gestures |
|
Brandtner [5]
|
1933 |
34
|
AVP
|
TP
|
_ |
médiane |
Suture simple |
|
Candy[11]
|
1956
|
14 |
Chute de sa motocyclette |
TP |
_ |
médiane |
HS :suture simple |
|
Hurlbut[12] |
1967 |
8 |
Chute d’un arbre |
TP |
- |
- |
- |
|
Herbert[13]
|
1973
|
7
|
Chute de sa bicyclette |
TP
|
_
|
Elective |
HS :suture simple |
|
IUCHTMAN[14] |
1997 |
7 |
Chute de sa bicyclette |
TP |
_ |
Elective |
HS :suture simple |
|
Che-Min Wu[8]
|
2006
|
63
|
AVP
|
TP
|
HS
|
Médiane
|
HSE + nécrose intestinle : Résection+suture |
|
Lopez[15] |
2010 |
14 |
Chute de sa bicyclette |
TP |
HS |
- |
- |
|
Thakur[4]
|
2013
|
9
|
Chute de sa bicyclette |
TP
|
HS
|
Elective |
HS : suture simple |
|
Aravinda[16] |
2014 |
38 |
Chute d’un arbre |
TP |
HS |
Médiane |
HSE :nécrose intestinale : Résection+stomie |
|
Brian Shea [17] |
2017 |
16 |
Chute de sa bicyclette |
Pas de TP |
HS |
Elective |
HS : suture simple |
|
Notre cas |
2017 |
23 |
agression |
Pas de TP |
HS+EP |
Médiane |
HSE : suture |
Conclusion
The diagnosis of post-traumatic spiegel hernia is difficult. The clinic may be lacking, hence the interest of an abdominal scanner that helps in the diagnosis. The immediate or deferred surgical management depends on whether or not the hernia is strangled and the associated abdominal lesions.
References
- Siddharth Y, Jain SK, Arora JK, Sharma P, Sharma A, et al. (2013) Traumatic abdominal wall hernia: delayed repair: advantageous or taxing. International journal of surgery case reports 4(1): 36-39.
- Al Beteddini Osama S, Abdulla S, Omari O (2016) Traumatic abdominal wall hernia: A case report and literature review. International journal of surgery case reports. 24: 57-59.
- Bansal S, Vyas KC (2015) Traumatic Abdominal Wall Hernia: A Case Report. Indian Journal of Surgery. 77(1): 193-194.
- Thakur SK, Gupta S, Goel S (2013) Traumatic spigelian hernia due to handlebar injury in a child: a case report and review of literature. Indian Journal of Surgery. 75(Suppl 1): 404-406.
- Brandtnes CE (1933) Uber einen fall von traumtischer uchdeckenhemie in der Linea Spigellii. Arch Orthop Unfall-Chir. 33: 219-221.
- Netto FACS, Hamilton P, Rizoli SB, Nascimento Jr B, Brenneman FD, et al. (2006) Traumatic abdominal wall hernia: epidemiology and clinical implications. Journal of Trauma and Acute Care Surgery. 61(5): 1058-1061.
- Hassan KA, Elsharawy MA, Moghazy K, AlQurain A (2008) Handlebar hernia: A rare type of abdominal wall hernia. Saudi Journal of Gastroenterology. 14(1): 33-35.
- Wu CM, Liu TH, Lin HJ, Wang GT (2006) Traumatic spigelian hernia. Injury Extra. 37: 404-406.
- Mzoughi Z, bayar R, Khmiri H, Gharbi L, Khalfallah MT (2016) Hernie post traumatique de la paroi abdominale antérieure. Pan African Medical Journal. 24: 203.
- Siddharth Y, Jain SK, Arora JK, Sharma P, Sharma A, et al. (2013) Traumatic abdominal wall hernia Delayed repair: Advantageous or taxing. Int J Surg Case Rep. 4(1): 36– 39.
- Candry RM. Traumatic hemia. Am J Surg (1956);91:301-303.
- Hurlbut HJ, Mosely T (1967) Spigelian hemia in a child. South Med J. 60(6): 602-605.
- Herbert RC, Turner FW (1973) Traumatic abdominal wall hemia in a 7-yearold child. J Pediatr Surg. 8(6): 975-976.
- Iuchtman M, Kessel B, Kirshon M (1997) Trauma-related acute spigelian hernia in a child. Pediatric emergency care. 13(6): 404- 405.
- Lopez, R., King, S., Maoate, K., & Beasley, S. (2010) Trauma may cause Spigelian herniae in children. ANZ journal of surgery, 80(9), 663-663.
- Aravinda PS, Saha S, Saurabh G, Andley M, Kumar A (2014) Traumatic Spigelian Hernia: A Rare Clinical Scenario. J Clin Diagn Res. 8(5): ND01-ND02.
- Shea B, Fasano G, Cohen IT (2017) Pediatric Spigelian hernia: A case report and review of the literature. Journal of Pediatric Surgery Case Reports. 21(C).