


Koyel Chakraborty, MD1*, Deepanjan Bhattacharya, MD2, Lokesh Saini, MD2
1Department(s) and institution(s) – Regional Institute of Ophthalmology, Medical College and Hospital, Kolkata
2Department(s) and institution(s) - Department of Pediatrics, Postgraduate Institute of Medical Education and Research, Chandigarh – 160012
*Corresponding Author: Koyel Chakraborty, MD, Department(s) and institution(s) – Regional Institute of Ophthalmology, Medical College and Hospital, Kolkata.
Abstract
Gillespie syndrome (GS) is a rare neurological disorder characterized by delayed developmental milestones, bilateral aniridia, and hypoplasia of cerebellar vermis. We report a 3 month old boy with developmental delay, bilateral aniridia, axial hypotonia and cerebellar vermis hypoplasia, based on which a diagnosis of Gillespie syndrome was made. He is the youngest patient to be reported till date.
Keywords: Developmental delay, nystagmus, aniridia
Case Report
A 3-month-old boy, second born to a non-consanguineous couple presented with jerky movement of eyeballs from the neonatal period. Perinatal history was uneventful; there was no history of abnormal body movements, poor feeding, or lethargy. He had a predominant motor delay in the form of poor neck control and visual fixation.
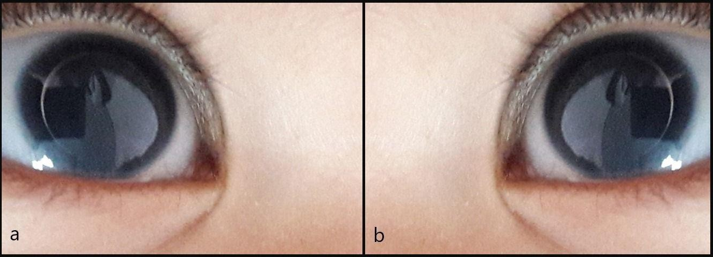
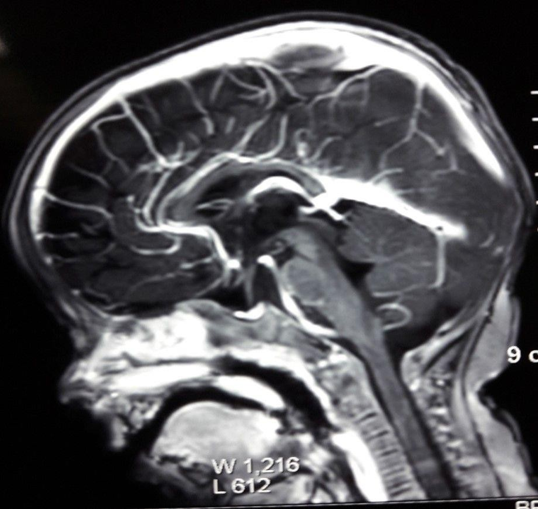
On general physical examination, he had normal head circumference and no evidence of dysmorphism. On ophthalmic examination, horizontal nystagmus with partially absent iris tissue and epicanthal folds were noted in both eyes (Figure 1). Systemic examination revealed marked axial hypotonia. External genitalia were normal, and there was no abdominal lump. Ultrasound of the abdomen showed bilateral normal kidneys. MRI brain revealed cerebellar vermis hypoplasia with mild atrophy of the bilateral frontal cortex (Figure 2). Based on bilateral partial aniridia, non-progressive cerebellar ataxia, and intellectual disability, along with delayed developmental milestones and axial hypotonia, a diagnosis of GS was made.
GS was first described by Frederick D Gillespie in 1965 [1] and less than 20 cases have been described worldwide, the youngest of whom is 5 months [2]. PAX6 gene mutations has been associated in few cases [3]. It has an autosomal recessive inheritance, though de novo mutations are more common. To our knowledge, this is the youngest case to be reported till date at 3 months of age.
The ophthalmic features of GS include festooned pupils, complete or partial aniridia, optic nerve hypoplasia, and pigmentary retinal changes. Non-progressive cerebellar ataxia manifests with delayed milestones and hypotonia in infancy and tremor and dysarthria in childhood. Dysmorphic features like a high forehead, hypertelorism, epicanthal folds, depressed nasal bridge, and thin upper lip may be present [4]. Other features include cerebellar hypoplasia and fusion of cervical vertebrae [5].
There is no established cure for this disease and prognosis depends on supportive management of disabilities.
Source(s) of support: Nil
Presentation at a meeting: Nil
Conflicting Interest (If present, give more details): Nil
Acknowledgement: None
References
- Gillespie FD (1965) Aniridia, cerebellar ataxia, and oligophrenia in siblings. Archives of Ophthalmology. 73: 338–341.
- Mariën P, Brouns R, Engelborghs S, Wackenier P, Verhoeven J, et al. (2008) Cerebellar cognitive affective syndrome without global mental retardation in two relatives with Gillespie syndrome. Cortex. 44(1): 54–67
- Glaser T, Ton CC, Mueller R, Petzl-Erler ML, Oliver C, et al. (1994) Absence of PAX6 gene mutations in Gillespie syndrome (partial aniridia, cerebellar ataxia, and mental retardation). Genomies. 19(1): 145-148.
- Online Mendelian Inheritance in Man, OMIM (TM). Johns Hopkins University, Baltimore, MD. MIM Number: {206700}: {04/18/2018}.
- Wittig EO, Moreira CA, Freire-Maia N, Vianna-Morgante AM (1988) Partial aniridia, cerebellar ataxia, and mental deficiency (Gillespie syndrome) in two brothers. Am J Med Genet. 30(3): 703-8.