


Wijerathne BPN 1, Sineka SHS2*
1Consultant General Surgeon, Teaching Hospital Kuliyapitiya, Sri Lanka.
2Intern Medical Officer, Teaching Hospital Kuliyapitiya, Sri Lanka.
*Corresponding Author: Sineka SHS, Intern Medical Officer, Teaching Hospital Kuliyapitiya, Sri Lanka.
Abstract
Introduction: Meckel’s diverticulum (MD) in inguinal hernia is a rare finding. This is known as Littre’s hernia. It is impossible to diagnose pre-operatively.
Presentation Of Case: we present a case of true Littre’s hernia in an incarcerated inguinal lump. The patient presented with a non-obstructive, painful right inguinal lump. During the inguinal hernia repair, an MD of 6.5cm Length was found tightly adhered to the hernia sac. The diverticula was resected, and the bowel loop was sutured and reduced into the peritoneum.
Discussion: MDs are usually overlooked. Therefore, it presents complications like infection, obstruction, or bleeding. Once diagnosed, surgical resection is recommended. Mesh appliance after resection is debatable.
Introduction
Meckel’s diverticulum (MD) is the most common form of malformation in the gastrointestinal (GI) tract. Typically, it is located in the ileum and can be seen in 2-4% of population [4]. Embryologically, it is a remnant of the fetus in various lengths.
Clinical presentations vary in MD. Usually, they are asymptomatic. Patients may present with any form of intestinal obstruction (Volvulus, intussusception, and hernia), PR bleeding, acute abdomen, appendicitis, or diverticulitis as a complication. Otherwise, the diagnosis is incidentally during imaging studies, laparotomies, or laparoscopies.
However, the diagnosis is overlooked due to the need for more specific clinical features. It is possible to diagnose a diverticulum by radiological methods such as barium studies, Ultrasound scans, and CT. Mesenteric angiograms help in the diagnosis of bleeding diverticula. Even though the findings are incidental, it is less cost- effective to use sophisticated investigations to discover asymptomatic diverticulum.
Surgical resection of symptomatic Meckel’s diverticulum is the treatment option. However, some surgeons prefer to dissect the diverticulum depending on the risk score as a guide. These include the patient’s age, Male gender, Length of diverticula, and fibrous band presence. We present a rare case of true incarcerated Littre’s hernia.
Case Study
A 42-year-old male patient presented with a right-side painful, irreducible inguinal lump for one-day duration. On further questioning, the lump was there for several months, which was not painful and reduced spontaneously. He did not have features of obstruction, such as vomiting, abdominal distension, and constipation. History was unremarkable otherwise.
He was afebrile and clinically ill on general examination. Blood pressure and other vitals were stable. Abdominal examination reveals no visible cough impulse in the right-side inguinal region with a soft and non-distended abdomen. Diagnosis of incarcerated inguinal hernia was made, and conservative management was, thinking of routine surgical repair later since he did not have obstructive features and had regular biochemical markers. USS abdomen was performed. It suggested an obstructed right-side inguinal hernia, and the pain was aggravating. Therefore, we proceeded to open inguinal hernia repair under spinal anesthesia.

Dissected finding of the Meckel’s diverticulum inside and tightly adhered to the hernia sac.
During the surgery, an indirect inguinal hernia with Meckel’s diverticulum tightly adhered to the hernial sac was found. Length of the MD was around 6.5cm and no duplications found in bowel. Meckel’s diverticulum dissected from it base with primary bowel repair and sample sent for histology. Bowel loop sutured and hernia sac excised. Bowel loop reduced in to peritoneum cavity. Posterior abdominal wall Darn repaired. Routine Lichtenstein repair not done since tissue was edematous to avoid mesh. Post-op was uneventful. Patient was discharged on post-operative day 3 with normal diet.
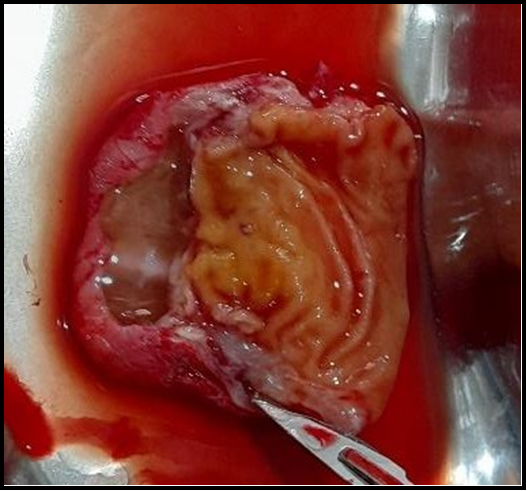
Cross section of the dissected hernia sac.
Discussion
Meckel’s diverticulum is seen in 2% of the population and is asymptomatic in 91-96% of people [1]. Hernia that contains Meckel’s diverticulum is a Littre’s hernia. Richter’s hernia has a traction diverticulum from the anti-mesenteric border of the intestine, which is a common mislead for diverticulum. Furthermore, Littre’s hernia is classified into two: “true” and “mixed,” with “true” having Meckel alone and “mixed” having a segment of small bowel other than Meckel’s. Here, in our case, we had a true Littre’s hernia, which is the commonest. [1].
Our case is an incarcerated Littre’s hernia, a rarer of 1% in the observed MD population [5]. However, 68 similar pediatric studies have been reported from the beginning of the 20th century to 2011 [2]. Few adult case studies were also noted [3,6].
There is a discussion about routine mesh appliances. Resection of diverticulum converts the clean inguinal surgery to clean contaminated surgery. Therefore, the risk of mesh getting infected is high. However, not applying mesh increases the risk of recurrence. In the literature, mesh infection accounts for 1%, and the recurrence with mesh is for 1-3%. Tissue repair is carried out in infected fields with a high recurrence rate of about 15%. [1]. Therefore, mesh placement should proceed after weighing the risks over the benefits for individual patients. However, the latest World Society of Emergency Surgery 2017 guidelines recommend mesh placement in clean, contaminated surgeries due to the low risk of infection. However, since it was a casualty and a young patient with an easy follow-up, we did not apply a mesh to the patient, thinking to address the concern later if a recurrence happens.
References
- Johnson GGRJ, Holden J, Helewa RM, Hochman D, Hyun E (2021) A strangulated meckel’s diverticulum in an inguinal hernia: A case report and literature review. International Medical Case Reports Journal. 14: 605–609.
- Pampal A, Aksakal ED (2011) Littre hernia in childhood: A case report with a brief review of the literature. African Journal of Paediatric Surgery. 8(2): 221–224.
- Pinto J, Viana CM, Pereira A, Falcão J (2019) Littré’s hernia. BMJ Case. 12(2).
- Sagar J, Kumar V, Shah DK (2006) Meckel’s diverticulum: Asystematic review. Journal of the Royal Society of Medicine. 99(10): 501–505.
- Şenol Z, Gülşen T (2021) A rare Meckel’s diverticulum complication in inguinal hernia: case report of Littre hernia. Anatolian Current Medical Journal. 3(1): 72–74.
- Stefanou SK, Stefanou CK, Paxinos AK, Tepelenis N, Kefala MA, et al. (2022) Littre Hernia in a 35 year old male: A case report. IOSR Journal of Dental and Medical Sciences (IOSR- JDMS). 21(9): 31–32.