


Diaby LM1*, Cisse MS1, Sanogo A1, Berthe BB1, Sanou MP2, Ndiaye M1, Sangare AS3, Niasse M2, Guindo OS4, Sangare S1, Guindo IK1, Ouologuem M1, Dembele G1
1Armed Forces Medical and Surgical Center of Bamako
2Cheikh Anta Diop University of Dakar
3Mali Hospital
4Hôpital de Sikasso
*Corresponding Author: Ladji Mohamed Diaby, Armed Forces Medical and Surgical Center of Bamako.
Abstract
Introduction: Osgood-Schlater disease is a painful inflammation of the bone and cartilage of the tibial tuberosity
Patients and methods: Our study took place in the Rheumatology unit of the Armed Forces Medical-Chirurgical Center of Bamako. This is a retrospective, cross-sectional study, carried out in patients followed from January 2021 to December 31, 2022. The study population was patients from the rheumatology unit, observations of the disease were included in our study. Of Osgood confirmed and excluded incomplete files which did not allow reliable use of the data.
Results: During our study period we collected 27 patients, i.e., 25 boys versus 2 girls. The age of the patients was in the range of 9 to 16 years. The majority of patients were male, i.e., 93%.
Discussion: For boys on average the pathology appears from 12 to 15 years old and in girls from 8 to 12 years old, with a prevalence of 9.8% (11.4% in boys, 8.3% in girls ).
Symptoms present bilaterally in 20% to 30% of patients. The damage was unilateral and the triggering factor was sport in the patients in this study.
Conclusion: osteoarticular disease is more common in adolescent males.
Keywords: Osgood-Schlater, Bamako
Introduction
Osgood-Schlater disease is a painful inflammation of the bone and cartilage of the tibial tuberosity [1-3] (figure 3). The disease is caused by excessive strain on the leg. Typical symptoms include pain, swelling and tenderness in the knee [3-6]. Osgood-Schlatter disease is osteochondrosis, which is a group of growth cartilage disorders that develop when a child grows rapidly [1-4].
Osgood-Schlatter disease appears between the ages of 10 and 15 and usually affects only one leg. It affects nearly 20% of sports children and 5 to 10% of non-sports children. The disease is generally more common in boys, but the gender gap is narrowing as more and more girls are involved in sports programmes [1-6]. The main symptoms of Osgood-Schlatter disease are pain, swelling, and tenderness in the tibial tuberosity at the front of the knee, just below the kneecap. Pain is aggravated by activity and reduced by rest [3].
The etiology of Osgood-Schlatter disease is said to be repeated and excessive traction of the patellar tendon (patellar tendon) where it is attached to the upper tibia. This upper tibial insertion point is called the tibial tuberosity. The diagnosis is based on a clinical examination and sometimes on X-rays. Treatment usually involves pain relief and rest [7].
The objective of this preliminary study is to evaluate the frequency of this pathology over twelve months at the Rheumatology Unit at the Armed Forces Medical and Surgical Center in Bamako.
Patients and Method
Scope of the study: Our study took place in the Rheumatology Unit of the Armed Forces Medical and Surgical Center in Bamako.
Type of study: This is a retrospective, cross-sectional study carried out in patients followed in the rheumatology unit
Study period: This is a preliminary study carried out between January 2021 and December 31, 2022.
Study population: was patients in the rheumatology unit,
Inclusion criteria: included in our study the observations of Osgood's disease confirmed by a standard X-ray
Criterion for non-inclusion: Other pathologies (osteochondrosis) of the tibial tuberosity
Exclusion criteria: And excluded incomplete files that did not allow reliable data exploitation.
Ethical aspects: The collection and use of patients' socio- demographic and clinical data was carried out in accordance with the rules of medical ethics regarding the anonymity of patients and the confidentiality of their data.
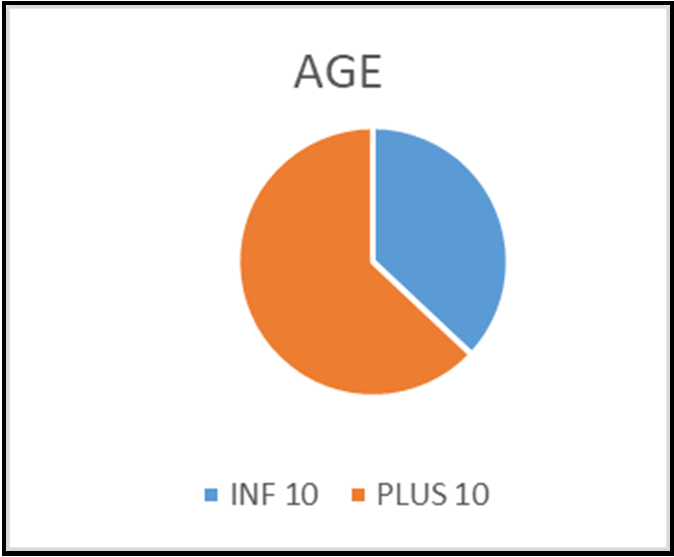
Figure 1: repartions des patients selon l’âge en deux tranches.
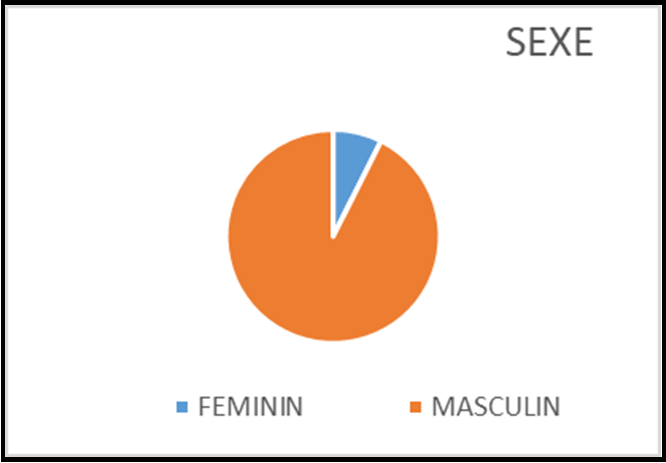
Figure 2: Répartition des patients selon le sexe

Figure 3: Profile knee X-ray showing tibial tuberosity detachment
The sex ratio was 12.5, the age range was 9 to 16 years and the mean age was 12.7 years.
In our study, all the disorders were monoarticular and the triggering factor was sport. The X-ray was the only imaging examination performed systematically. The basis of treatment was rest associated with the intake of analgesic (paracetamol).
Patients were regularly followed up at one month, then at 3 months and at 6 months. Clinically, there was a clear improvement and at 6 months there were more radiological lesions.
Discussion
During our study period, we collected 27 patients. The ages of the patients ranged from 9 to 16 years (Figure 1). The patients were male (25 cases), i.e., 92.59% compared to 7.41% for the female sex (Figure 2). These data are generally mentioned by the literature, which leans towards a more frequent involvement of the male sex [1,3,8], but also frequent in adolescence [8].
For boys on average, the disease occurs between the ages of 12 and 15 and for girls from 8 to 12 years of age, with a prevalence of 9.8% (11.4% in boys, 8.3% in girls) [7,8].
Symptoms present bilaterally in 20% to 30% of patients. The involvement was unilateral and the triggering factor was sport in the patients in this study.
A study carried out in Mali between 2006 and 2008 found 7 cases including 3 girls and 4 boys with a mean age of 13 years and the bilateral form represented 57.14% [8]
In our case, all patients had an X-ray of the affected knee which confirmed the diagnosis. MRI has not been performed in patients due to its cost and availability. In other similar studies, X-ray was the most performed examination, followed by MRI to further study the insertion of the tendon [1-5]. For management, all patients have observed rest, benefited from paracetamol without any contraindications and this treatment in the literature is the basis of treatment and is often associated with anti-inflammatory drugs [1- 3,7,8,9]
Conclusion
Osgood-Schlater disease is a pathology of tibial cartilage and is common in adolescent males. Its diagnosis is clinical-radiological and the basis of treatment is the use of analgesics and appropriate rest.
References
- Vargas B, Lutz N, Dutoit M, Zambelli PY (2008) Maladie d’Osgood-Schlatter. Rev Med Suisse. 172(6): 2060-2063.
- Vaishya R, Azizi AT, Agarwal AK, Vijay V (2016) Apophysitis of the Tibial tuberosity (Osgood-Schlater Disease): A review. Cureus. 8(9): e780.
- Danneberg DJ (2017) Successful Treatment of Osgood-Schlater Disease with Autologous-Coditioned Plasma in two Patients. Joint. 5(3): 191-194.
- Beaubois Y, et al. Osgood-Schlatter disease: from sports cessation to the management of biomechanical disorders. Kinesither Rev (2016).
- Corbi F, Matas S, Álvarez-Herms J, Sitko S, Baiget E, et al. (2022) Osgood-Schlatter Disease: Appearance, Diagnosis and Treatment: A Narrative Review. Healthcare (Basel). 10(6): 1011.
- Mun F, Hennrikus WL (2021) Surgical Treatment Outcomes of Unresolved Osgood-Schlatter Disease in Adolescent Athletes. Case Rep Orthop. 2021: 6677333.
- Poboży T, Konarski W, Piotrowska-Lis K, Domańska J, Poboży K, et al. (2022) Basic Differences and Most Common Findings in Ultrasound Examinations of Musculoskeletal System in Children: A Narrative Literature Review. Healthcare (Basel). 10(10): 2010.
- Drissa B (2010) Epidemiological; clinical; radiological and therapeutic aspects in the Rheumatology Department at the University Hospital of Point G (Mali), USTTB medical thesis Bamako.
- Schrouff I, Magotteaux J, Gillet P (2015) Comment je traite ... la maladie d'Osgood-Schlatter [How I treat ... Osgood-Schlatter disease]. Rev Med Liege. 70(4): 159-62.