


Mohamad Hafiz Mohmad Hassim, MsOrtho*, Norhaslinda Bahaudin, MsOrtho, Meghan Balakumaran, MD, Abdul Rauf Ahmad, MsOrtho
Department of Orthopaedic, Traumatology & Rehabilitation, Hospital Tuanku Ja’afar Seremban, Malaysia
*Corresponding Author: Mohamad Hafiz Mohmad Hassim, MsOrtho, Department of Orthopaedic, Traumatology & Rehabilitation, Hospital Tuanku Ja’afar Seremban, Malaysia.
Abstract
Context
Application of WALANT (Wide Awake Local Anesthesia No Tourniquet) technique to more minor procedures to achieve good results for post- limb reconstruction-related surgeries during the outbreak of Covid-19.
Aims
To reduce the general and regional anesthesia elective operation burden list for post-limb reconstruction adjunct procedures.
Methods and Material
10 patients were selected, with 9 undergoing bone-related procedures and 1 for soft tissue procedures. Standard WALANT solution was diluted with a maximum safe limit of 7mg/kg for lidocaine, and epinephrine or 40mls of the cocktail is strictly adhered to prevent complications. Visual Analogue Scale (VAS) was used to evaluate pain before, during, and after the procedure for up to 6 hours.
Statistical analysis used
Statistical analysis using SPSS version 25 to calculate significant correlation between the VAS pain score and time interval before solution injection till 6 hours postoperative.
Results:
5 patients underwent chipping osteotomy, 4 underwent corticotomy, and 1 for invaginated skin release procedure. The mean VAS pain score was calculated and showed nearly zero (0) score during the operations, with the highest mean pain score recorded at a maximum of 4.5 after 6 hours postoperatively.
Conclusions:
WALANT technique in lower limb post-reconstruction adjunct procedures was an option during the COVID-19 pandemic as it is proven safe and effective.
Keywords: WALANT, lower limb reconstruction-related procedures, visual analog scale
Introduction
Dr. Donald Lalonde [1,2] popularises WALANT (Wide Awake Local Anesthesia No Tourniquet) technique. It has been used widely for elective and trauma hand surgeries in the outpatient setting since a decade ago. This method allows local anesthesia and analgesia to be given directly to the operative site containing lidocaine and epinephrine [3]. The advantages and uniqueness of WALANT are that all patients were exempted from preoperative clearance, fasting before the surgery, and also to withhold patients' regular medication. Not having to use a tourniquet throughout the procedure voids potential nerve damage and pain from limb ischemia. Since the WALANT technique was first accepted, it became widely used and expanded further towards fracture fixation, such as in procedures involving the phalanges of the finger, distal end radius, and clavicle. Li et al. [4], Bilgeteken et al. [5], and Poggetti et al. [6] conducted lower extremities procedures, either fracture fixation or soft tissues procedure over the ankle region using WALANT and reported significantly reduced postoperative pain with no complications.
Limb reconstruction adjunct procedures following the Ilizarov principles for the law of distraction osteogenesis are frequently done to address problems, obstacles, and complications related to Ilizarov surgeries. Distraction osteogenesis (DO) is a surgical technique in which the intrinsic capacity of bone to regenerate is harnessed to lengthen bones or to replace large segments of bone. It consists of applying an external fixator to the affected bone, followed by an osteotomy of the bone, and then gradual and controlled distraction is used to the two bone segments [7]. Russian surgeon Gavril Ilizarov, who pioneered the biological principles of bone and soft tissue regeneration and popularized the technique of distraction osteogenesis, discovered that a new bone would regenerate in the distracted gap under slow and gradual distraction, which will further consolidate and remodel to become matured bone.
In limb reconstruction procedures, a few problems might arise over the course of treatment, especially in the bony union over the docking site for bone transport surgeries and while awaiting skeletal regeneration to fully consolidate, as well as skin infolding preventing the docking site from approximating. There are techniques to overcome this problem, such as skin release for invaginated skin, corticotomy for bone lengthening, chipping osteotomy, and bone grafting for delayed union in the docking site area once the bone transport is completed.
Most of the above procedures were done under general or regional anesthesia, which required the anesthetic team to be involved. During covid-19 pandemic, all of the operating procedures requiring anesthesia were prioritized to the emergency procedure for both Covid-19 and non-Covid-19 patients. This causes a tremendous decrease in operating slots resulting in a backlog of these procedures as elective operating lists. In light of the success of WALANT surgery on minor upper limb and lower limb procedures done in our center, we expand the use of WALANT surgery to be applied for limb reconstruction-related minor procedures.
Subjects and Methods:
In 2021, during the onset of the pandemic Covid-19 at Hospital Tuanku Jaafar, Seremban, Negeri Sembilan, Malaysia, we faced difficulties performing post-lower limb reconstruction surgeries under general anesthesia due to less priority given to these minor procedures. However, these procedures, especially corticotomy for early consolidation of the regenerate segment and skin release for invaginated docking site, will significantly impact the union and outcome of the treatment if it is not done in due time. Given this, we decided to use the WALANT techniques substitutes for general and regional anesthesia. The objectives of using WALANT in these procedures are to reduce cases listed under general or regional anesthesia during the COVID-19 pandemic and evaluate the effectiveness of WALANT during the process based on the Visual Analogue Scale (VAS).
Most of the procedures included were minor and could be done within 30 to 60 minutes. The methods selected to be done under WALANT are divided into two groups. One group for soft tissue procedures such as skin release for invaginated skin. Another group for a bone-related procedures such as corticotomy for bone lengthening, re-corticomy for early consolidation, and chipping osteotomy over the docking site in bone transport.
Absolute contraindications using WALANT for minor procedure post lower limb reconstruction include conditions associated with vascular diseases, sickled erythrocytes, abnormal clotting profiles or bleeding disorders, and anxious or non-cooperative patients. At the same time, relative contraindications include those with active infection and morbid obesity.
All the selected patients were admitted on the day of the surgery itself, the patient did not fast, and the procedures were done in a sterile operation theatre without an anesthetist. Standard WALANT solution was diluted to a 2:1 ratio using 50cc 0.9 % normal saline, 50cc 2 % lidocaine, 10cc 8.4% sodium bicarbonate, and 1mg 0.18% epinephrine acid tartrate (Figure 1). The maximum safe limit of 7mg/kg for lidocaine and epinephrine or 40mls of our cocktail is strictly adhered to prevent complications.

Figure 1: WALANT solution
The solution was injected in all directions 15 to 30 minutes before the skin incision. Depending on the procedures and site involved, the cocktail infiltration usually follows a marked skin incision up to 0.5cm circumferentially, and once deeper dissection is reached, the cocktail is reintroduced subperiosteally (Figure 2).

Figure 2: WALANT solution injected at surgical area. (a) tibia bone procedure, (b) femur bone procedure
In bone-related procedures, either chipping osteotomy or corticotomy, C-arm was used to locate the area precisely, so it can prevent multiple attempts and might cause patient pain throughout the procedure (Figure 3). Otherwise, in skin release for invaginated skin, the process involved only soft tissue from the superficial to the deep tissues (Figure 4).
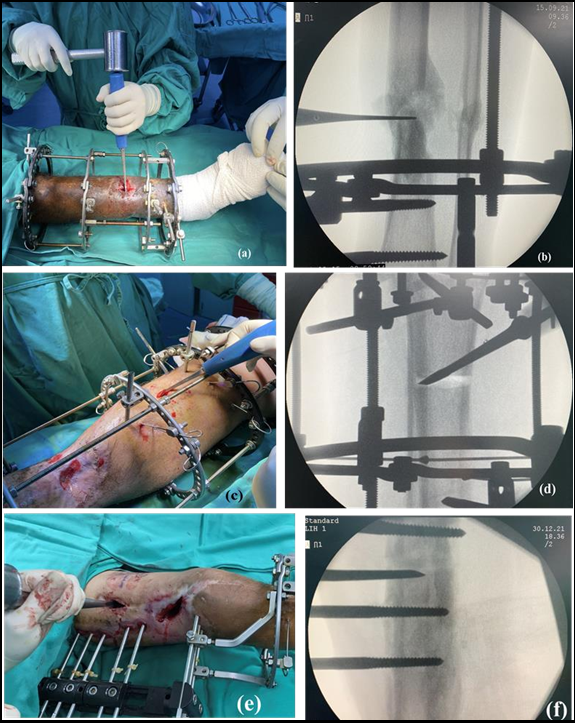
Figure 3: Bone related procedures; (a) Chipping Osteotomy of tibia, (b) Imaging Intensifier guidance for procedure in (a), (c) Corticotomy of tibia, (d) Imaging Intensifier guidance for procedure in (c), (e) Corticotomy of Femur, (f) Imaging Intensifier guidance for procedure
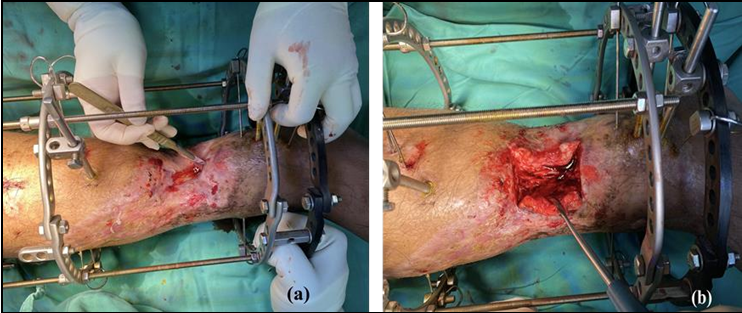
Figure 4: Invaginated skin release (a) incision area, (b) after completed the skin release
A visual Analogue Scale (VAS) was used to evaluate the pain. It was documented for monitoring the pain from before the procedure, while the solution was injected, throughout the process, and up to 360 minutes (6 hours) postoperatively (Figure 5).
Statistical analysis using SPSS version 25 calculates the significant correlation between the VAS pain score and the time interval from the solution injected to 6 hours postoperative. The mean VAS pain score was also calculated for all the procedures.
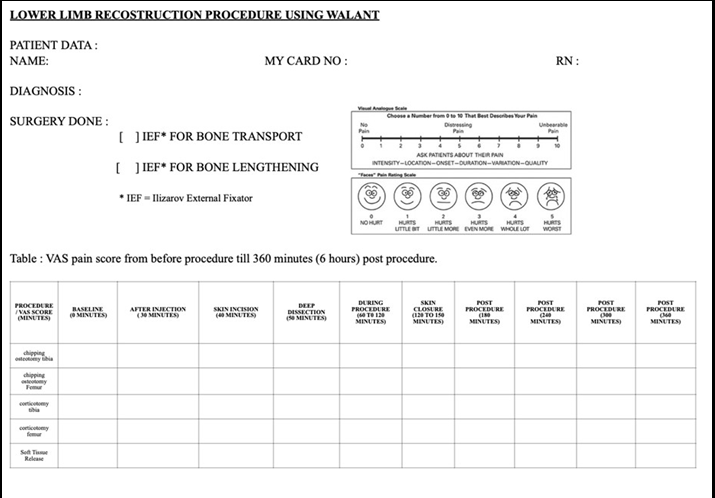
Figure 5: Form for demographic data, type of procedure with VAS score
Results
A total of 10 patients agreed and consented to involve in post-limb reconstruction procedures using the WALANT technique from January to December 2021. Out of 10 patients, 9 patients underwent the bony procedure, and only 1 patient for the soft tissue procedure. For bony procedures, 5 patients underwent chipping osteotomy of the tibia, 2 for bone lengthening corticotomy of the tibia, and another 2 for bone transport corticotomy of the femur. The soft tissue procedure is mainly for the release of invaginated skin. The VAS pain score was documented in each course, and the mean was calculated (Table 1, 2).
The mean VAS pain score for the total bone procedure was calculated (Table 3). The statistical correlation between the mean VAS pain score with the duration before and after the injection of the WALANT solution was also computed using SPSS version 25 and plotted in the graph (Figure 6). However, it does not show a significant correlation.
None of the 10 patients reported developing any lidocaine toxicity throughout the procedure after being given the WALANT solution. All the procedures did not cause much bleeding.
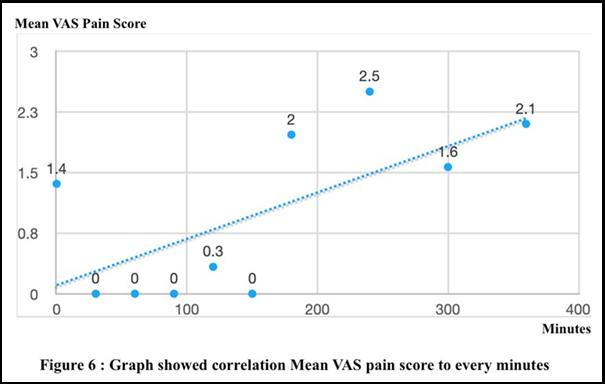
Table 1: Mean VAS for bone procedure from before the procedure till 6 hours (360 minutes) post procedure
|
Procedure / Minutes |
Baselin e (0) |
After Injection (30) |
Skin incision (40) |
Deep Dissection (50) |
During Procedure (60 to 120) |
Skin Closure (120 to 150) |
Post Procedure (180) |
Post Procedure (240) |
Post Procedure (300) |
Post Procedure (360) |
|
chipping osteotomy tibia |
1.6 |
0 |
0 |
0 |
0 |
0 |
2.4 |
2 |
1.2 |
1.8 |
|
corticotomy tibia |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
2 |
1 |
1 |
|
corticotomy femur |
2.5 |
0 |
0 |
0 |
0 |
0 |
2.5 |
3.5 |
2.5 |
4.5 |
Table 2: Mean VAS for Soft tissue procedure from before the procedure till 6 hours (360 minutes) post procedure
|
Procedure / Minutes |
Baseli ne (0) |
After Injection (30) |
Skin incision (40) |
Deep Dissection (50) |
During Procedure (60 to 120) |
Skin Closure (120 to 150) |
Post Procedure (180) |
Post Procedure (240) |
Post Procedure (300) |
Post Procedure (360) |
|
Skin release for inviginated skin at tibia |
0 |
0 |
0 |
0 |
0 |
0 |
1 |
2 |
1 |
1 |
Table 3: Mean pain score (VAS) for total bone procedure monitoring after given WALANT
|
Minutes |
Mean Pain score (VAS) |
|
0 |
1.36 |
|
30 |
0 |
|
60 |
0 |
|
90 |
0 |
|
120 |
0.333 |
|
150 |
0 |
|
180 |
1.967 |
|
240 |
2.5 |
|
300 |
1.567 |
|
360 |
2.1 |
Discussion
WALANT is widely used for upper limb surgeries, and the advantages of this method give patients more satisfaction and the success of the procedures themselves. In lower limb procedures, mainly over the ankle and foot region, usage of WALANT solution in fracture fixation or soft tissue repair has minimal data and studies available.
Used of WALANT was experimented with in light of the Covid-19 pandemic as operating time shortage is inevitable but with success. Apart from the simple fixation of upper limbs and lower limbs, the other frequently left out procedures are post lower limb reconstruction-related procedures, to overcome either the obstacles, complications, or even secondary procedures from limb reconstruction surgeries. These procedures include corticotomy, bone chipping, and release of skin invagination. This is the first case series of limb reconstruction-related procedures of long bones, such as the tibia and femur, done under WALANT.
Almost all 10 patients in our case series had a mean VAS pain score of 2 and below. The most critical pain evaluation during the procedure, which was evaluated around 60 minutes to 90 minutes, produced a score of zero (0) in all 10 patients. This data concludes that the WALANT technique can be applied in deep or extensive bone procedures. The injection technique of WALANT solution to cover all surfaces of the periosteum was the key to the success of this procedure.
Even though statistical calculation using SPSS version 25 did not show a significant correlation, it is most likely due to a minimum number of case series included in the sample. However, we believed the pain experienced by all the patients was minimal, even at 6 hours postoperatively.
As the pandemic Covid-19 situation worsened, many post-limb reconstructions, especially bone transport procedures, faced complications, either invaginated skin or poor union progress at the docking site requiring minor procedures. These were put to a halt due to restricted operating time. If it's not done, this timely intervention will prolong the external fixator time and development complications related to prolonged external fixator duration, such as pin tract infection and joint stiffness, thus creating a vicious cycle.
The WALANT technique aids tremendously and provides a solution to overcoming the overload cases that require general or regional anesthesia. The surgery can be done earlier, eliminating anesthetist risk as they are facing shortage during the pandemic, besides eliminating tourniquet complications and bleeding during the procedure. This method further benefits the anesthesia team because they can spend more time with Covid-19 patients who need emergency operations or attention. Another key to success in this case series is proper patient selection, which is crucial, and indication and contraindications should be strictly scrutinized.
Conclusion
WALANT is a good alternative and successful option for surgical procedures to be done apart from general anesthesia. Pandemic Covid-19 halted most elective surgical procedures due to prioritization given to the emergency and covid cases and the shift of total anesthesia workload towards intensive care away from surgeries.
The lower limb post-reconstruction procedure is a procedure that needs to be performed at a specific time to achieve a good result for the patient to be able to perform their activity of daily living independently. WALANT is a significant dilution and solution to the first combination in lower limb post-reconstruction-related procedures. Patient selection and doctor-patient communication are also crucial for this procedure's success.
Key Messages
The usage of WALANT as an alternative to general or regional anesthesia has successfully evolved following the global reduction in elective operative slots during Covid 19 pandemic from hand surgeries towards more diverse surgeries involving adjunct limb reconstruction procedures as it is proven safe and efficient with careful patient selection.
References
- Lalonde D, Bell M, Benoit P, Sparkes G, Denkler K, et al. (2005) A multicenter prospective study of 3,110 consecutive cases of elective epinephrine use in the fingers and hand: The Dalhousie Project clinical phase. J Hand Surg Am. 30(5): 1061–1067.
- Lalonde D, Martin A (2013) Epinephrine in local anesthesia in finger and hand surgery: the case for wide-awake anesthesia. J Am Acad Orthop Surg. 21(8): 443–447.
- Lalonde DH (2010) “Hole-in-one” local anesthesia for wide- awake car- pal tunnel surgery. Plast Reconstr Surg. 126(5): 1642– 1644.
- Li YS, Chen CY, Lin KC, Tarng YW, Hsu CJ, et al. (2019) Open reduction and internal fixa- tion of ankle fracture using wide- awake local anaesthesia no tour- niquet technique. Injury. 50(4): 990–994.
- Bilgetekin YG, Kuzucu Y, Öztürk A, Yüksel S, Atilla HA, et al. (2020) The use of the wide- awake local anesthesia no tourniquet technique in foot and ankle injuries. Foot Ankle Surg. 27(5): 535- 538.
- Poggetti A, Del Chiaro A, Nicastro M, Parchi P, Piolanti N, et al. (2018) A local anesthesia without tourniquet for distal fibula hardware removal after open reduction and internal fixation: the safe use of epinephrine in the foot. A randomized clinical study. J Biol Regul Homeost Agents. 32(6 suppl 1): 57–63.
- Hamdy RC, Rendon JS, Tabrizian M (2012) Distraction Osteogenesis and Its Challenges in Bone Regeneration, Bone Regeneration. Prof. Haim Tal (Ed.), ISBN: 978-953-51-0487-2, InTech.