


Kumar Raj Ranjan*
Durgapur Steel Plant Hospital & Research Centre, Dist- Bardhaman, West Bengal.
*Corresponding Author: Kumar Raj Ranjan, Durgapur Steel Plant Hospital & Research Centre, Dist- Bardhaman, West Bengal.
Abstract
Gallstone disease (GSD) is the most common clinical problem requiring surgical intervention. The reported incidence of gallstones increases with age and is more common in females than males. GSD may remain asymptomatic in most cases, or patients may present with acute cholecystitis, chronic/recurrent cholecystitis, jaundice, cholangitis, and pancreatitis. Cholesterol supersaturation remains at the heart of gallstone formation.
Keywords: Multiple gallstones, acute and chronic cholecystitis, cholecystectomy, gallbladder cancer.
Introduction
Cholelithiasis is a chronic, recurrent disease of the hepatobiliary system. The impaired cholesterol, bile acids, and bilirubin metabolism are responsible for gallstone formation. The prevalence of gallstones varies and has been reported as 2-29% in India and has been increasing in recent years. About 10% of the population in Western countries harbor gallstones, an epidemic in some areas, while its incidence is low in Asia. Women are more commonly affected than men. There are two broad classes of gallstones: cholesterol and pigment stones. Cholesterol supersaturation of bile lies at the heart of gallstone formation. Pigment stones are formed due to hemolytic conditions. [1]. The risk factors leading to gallstone formation include fertile females, obesity, increasing age, and complex interplay of environmental, genetic, and metabolic syndrome [2]. Gallstones may be asymptomatic in most cases or present with acute cholecystitis, chronic/recurrent cholecystitis, cholangitis, jaundice, and pancreatitis [3]. Long-standing gallstones can lead to gallbladder cancer due to constant irritation of the mucosal layer [4]. It is rare to have hundreds of gallstones, and this condition is scarcely reported in the literature. We describe a thickened and fibrosed gallbladder with hundreds of gallstones inside (425).
Case Presentation
A 52-year-old male presented with right upper quadrant abdominal pain radiating to his back and vomiting for two days’ duration. He looked sick, with BP- 120/70mmHg, HR- 96bpm, and temperature- 100-degree Fahrenheit. He was non-icterus and had Morphy sign positive. Blood workup showed leucocytosis with left shift (TLC=16300, Neutrophils = 90%). He was treated with antibiotic (inj. Ceftriaxone), analgesic and omeprazole). Ultrasonography was performed, which showed multiple small stones in the gallbladder. We did laparoscopic cholecystectomy and encountered a thickened fibrous gallbladder [Figure 2] wall with 425 stones of size ranging from 5mm to 1cm inside it [Figure 1].
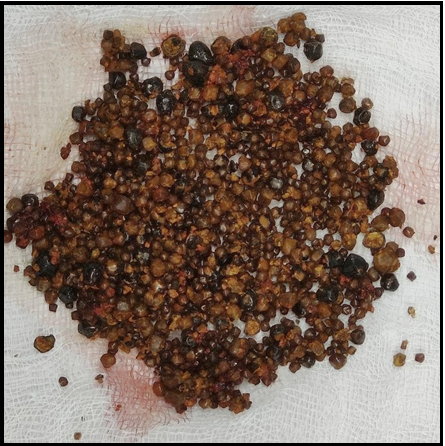
Figure 1: Multiple gallstones retrieved during laparoscopic cholecystectomy.

Figure 2: Sectioned thickened gallbladder.
Discussion
Gallstone disease is the most prevalent hepatobiliary disorder. Management of gallstones and their complications incurs significant financial burden [5]. Age and sex are considered vital risk factors [6,7]. Multiple stones and age are strong predictors of complications. An estimated 20% of adults over 40 years and 30% of over 70 years of age have biliary calculi. The risk factors responsible for gallstones include obesity, diabetes mellitus, estrogen, pregnancy, hemolytic diseases, and liver cirrhosis. The cholesterol stones are more common (75%), and the rest are pigment stones. The clinical presentation includes moderate to severe pain, vomiting, nausea, fever, and jaundice. Roa et al. [3], in their study, showed that 76% of patients with gallbladder cancer harbor multiple stones, while those with benign diseases have few or solitary stones. Bile culture for bacteria is positive in 30% of cases of gallstones. E. coli and Klebsiella are most commonly found in bile culture. Domeyer and Sergentanis, in their study, found that older patients had multiple small stones. Solitary stones and younger age were the most prominent predictors of severe inflammation. Multiple gallstones are associated negatively with the degree of inflammation [8]. However, our patient had a high degree of inflammation and a history of recurrent symptoms, and there were hundreds of stones found, and counted about 425 stones, sizes ranging from 5mm to 1cm. Our patient is older and has multiple stones with severe inflammation. Ultrasonography remains the most commonly performed diagnostic tool and is considered the test of choice, although additional imaging studies may be required [9,10]. Surgery is the mainstay of management for symptomatic gallstones and in the selected condition of asymptomatic cases. If the gallbladder is complicated with infection, it should be treated with broad-spectrum antibiotics, followed by interval cholecystectomy [11]
Conclusion
Diagnosis is not straightforward, as gallstone diseases can mimic various other illnesses. The relevance of this case report is due to the large number (425) of gallstones removed through laparoscopic cholecystectomy. This case is among the large number of gallstones retrieved laparoscopically in India.
Conflict of Interest: None declared.
Ethical Approval: Exempted by our institution.
Patient consent: Informed written consent obtained from patient for publication.
Fund & Sponsorship: Nil.
References
- Marshal HU, Einarsson C. Gallstone disease. J. Intern Med.2007;261(6):529-42.
- Yoo EH, Lee SY. The prevalence and risk factors for gallstone disease. Clin. Chem Lab. Med. 2009;47(7): 795-807.
- Roa I, Ibacache G, Roa J, Araya J, Aretxabala X de, Munoz S. Gallstone and gallbladder cancer-volume and weight of the gallstones are associated with gallbladder cancer: A case-control study. J Surg Oncol. 2006;93 (8)624-8.
- Vitella L, Sali A, Little P, Mrazek L. Gallstone andgallbladder carcinoma. Aust N Z J Surg2000;70(9): 667-73.
- Shaffer EA, Epidemiology and risk factors for gallstone disease: Hasthe paradigm changed in the 21th century? Curr Gastroenterol Rep.2005;7(2):132-40.
- Diehl AK. Epidemiologyand natural history of gallstone disease. Gasrtoenterol Clin North Am. 1991;20(1): 1-19.
- Halldestam I, Kullman E, Borch K, Incidence of and potential risk factors of gallstone disease in a general population sample. Br J Surg.2009;96(11):1315-22.
- Domeyer PJ, Sergentanis TN, Zagouri F, Tzilalis B, Mouzakioti E, Parasi A, et al. Chronic chloecystitis in elderly patients. Correaltion of the severity of inflammation with the number and size of the stones. In Vivo. 2008;22(2):269-72.
- MacDonald AA, Richardson M, Sue L, Hakwai A, Stephenson G, Harman R, et al. Beside ultrasonography for acute gallstone disease: a diagnostic accuracy study of surgical registrars and emergency medicine physicians. ANZ J Surg. 2020;90(12):2467- 71.
- Cremer A, Arvanitakis M. Diagnosis and management of bile stone disease anditscommplications. Minerva Gastroenterol Dietol. 2016; 62(1):103-29.
- Portincasa P, Di Ciaula A, de Bari O, Garruti G, Palmieri VO, Wang DQH. Management of gallstones and its related complications. Expert Rev Gastroenterol Hepatol. 2016; 10(1): 93-112.