


Suha Salah Algain1, Mohammed Alsuwaidan2, Salem D. Alsuwaidan3*, Fahad Fawzi Al-Deaji4
1Family Medicine Academy department, King Saud Medical City, Ministry of Health, Riyadh, KSA
2Ministry of health, Primary care agency
3Research and Innovation center, King Saud Medical City, Ministry of Health, Riyadh, KSA
4assistant consultant in critical care medicine, Prince Mohammed bin Abdulaziz hospital, Ministry of health, Riyadh, KSA
*Corresponding Author: Salem D. Alsuwaidan, Research and Innovation center, King Saud Medical City, Ministry of Health, Riyadh, KSA
Abstract
Introduction: The referral system is the most effective model for linking and integrating medical services across the three levels of care. It helps deliver cost-effective, high-quality care to our health consumers. In Saudi Arabia, the referral system is established on guidelines that clearly describe the referral process, incorporating a predesigned, standardized referral letter with significant, relevant, clinical, and social information about the patient.
Objective: This study may help improve the referral system and provide an important opportunity for shared understanding, enhanced knowledge, and effective learning of all participants. This study aimed to implement future changes in primary healthcare centers (PHCCs) to improve the referral process and overall quality of care.
Methodology: This quantitative research collected data from three Saudi board-accredited PHCCs and cluster 1 Riyadh, Ministry of Health referral records. This study excluded dental and family medicine clinic referrals at secondary level hospitals; the rest of the specialties were included.
Result: This study was conducted on 799 referrals from PHCCs. Results were collected from three main PHCCs, namely, Al-Malaz PHC with 51 (6.4 %) referrals, Laban PHC with 385 (48.2 %) referrals, and Tweeq Al-Qarbi with 363 (45.4 %) referrals. These referrals had different types; most of them were elective 768, 96.1 %), immediate (9, 1.1 %), and urgent (22, 2.8 %) referrals.
The most frequently referred specialty was internal medicine with 163 (20.4 %) referrals, followed by obstetrics and gynecology (134, 16.8 %), orthopedics (104, 13 %), and general surgery (89, 11.1 %), and dermatology clinic (81, 10.1 %).
Conclusion: The most commonly referred specialty was internal medicine. Notably, dermatology was among the top five referred things, thereby considered substantial by others. The referral process should be revised and consider the less essential referrals. Most importantly, a specialized clinic should be established for the most commonly referred specialties such as internal medicine, obstetrics and gynecology, and orthopedics.
Keywords: guideline, PHC, referral, healthcare system.
Introduction
The referral system is one of the most effective models for linking and integrating medical services across the three levels of care. It facilitates delivering cost-effective, high-quality care to our health consumers [1]. Most developed countries classify the health system into three health facilities: primary, secondary, and tertiary. The Ministry of Health has introduced a referral system in which all patients must seek care first at the primary healthcare centers (PHCCs) and then be evaluated and referred if they need a secondary level of care; in this way, patients are assured of receiving better care in the closest healthcare setting to their home and to have better cost-effective utilization of the health services. In Saudi Arabia, the referral system is established on clear guidelines describing the referral process. It incorporates a predesigned, standardized referral letter containing the patient's significant, relevant, clinical, and social information, which should be filled by the primary healthcare (PHC) physician [2].
In a previous study, the rate of referrals from PHCC to secondary healthcare indicated either no or insufficient information feedback to the PHC physicians [3]. In addition, the lack of knowledge and practice of referral systems in urban and rural PHCCs was unacceptable [4]. The absent or inadequate feedback from hospitals receiving referrals from PHCC indicates no continuum of critical information about patients referred to hospitals, thereby ineffectively improving the quality of care and possibly leading to wastage of resources [5].
Decreased efficacy was also found with the "Mawid or Ehalati" referral system in PHCC, which needs improvement in numerous factors, including the appointment time, physician practice, and feedback, for a better patient journey [6]. More studies have shown several weak points of the referral system, and many challenges have been identified; nonetheless, they have provided suggestions, such as implementing e-referral and Lean Six Sigma principles, to improve the quality of the referral system [7,8,9].
The ideal referral template letter should contain the physician's name, the reason for the state of the referral (urgent or routine), and a feedback space. The referring physician should explain the reason for referral in the referral letter, and the patient should diligently adhere to the instructions of the PHCC physician; in turn, the physician referred to should provide clear feedback to the referring physician. This whole effort often ends in a successful referral and provides an important opportunity for shared understanding, improved knowledge, and effective learning of all participants [10,11,12]. Some reasons for referral include emergency cases that cannot be managed at the PHCC, uncertainty in diagnosis, the need for further investigations that are not available at the PHCC, tension with the management options, and personal request by the patient [13]. With continuous identification of the challenges and constant suggestions for referral system efficiency, the referral processes conducted by the healthcare professionals would be improved.
This study aims to evaluate the referrals and, hopefully, find ways to reduce unnecessary referrals from PHCCs to secondary hospitals. The findings will help implement future improvements in PHCC to enhance the referral system and the quality of care provided to the patients. The impact of this study is to identify the most commonly referred specialties and determine the most common diagnosis of the referral cases from the PHCCs. This study will advocate the authorities in planning specific guidelines for the PHC referrals. The primary objective of this study is to estimate the rate of referrals from PHCCs to secondary hospitals, followed by identifying the most frequently referred specialties and the most common diagnosis of the referral cases.
Methodology
This observational, cross-sectional study measured the rate of referrals from PHCCs to secondary healthcare hospitals and subspecialized clinics at other PHCCs. This study was conducted in three accredited PHCCs under cluster 1 in Riyadh, Saudi Arabia, with 799 referral letters.
Data were collected in an Excel sheet and sorted by the PHCC referral records containing the word "letters." The papers were randomly selected from all of the abovementioned clinics. The authors viewed each referral form to ensure that the referral form met the inclusion criteria of a referral to all specialties. Referrals to secondary hospitals' dental and family medicine clinics were excluded, given that these clinics mainly refer to unnecessary referrals.
The main variables to be measured were the type of referral (immediate, urgent, or elective), the provisional diagnosis of the referred case, and the reason for referral (e.g., diagnosis and management, general checkup, upon patient's request, follow-up, and annual checkup).
Furthermore, this study included all referrals from specialties at secondary hospitals and subspecialized clinics at other PHCCs.
Statistical Considerations:
The number of referrals per PHCC, personal data (age and sex), referred specialty, referral type, provisional diagnosis, and referral reason were examined by descriptive analysis. These data were checked for accuracy and analyzed accordingly.
Results
799 referrals from PHCCs to a tertiary care hospital were found. More than half of the studied cases were female (473, 59.2 %) compared with male (326, 40.8 %). The mean age was 38.8 (±15.1, standard deviation [SD]). Results were collected from three main PHCCs, namely, Laban PHC, Tweeq Al-Qarbi, and Al-Malaz PHC, with 385 (48.2 %) and 363 (45.4 %), 51 (6.4 %) referrals, respectively. Regarding referral type, majority were elective referrals (768, 96.1 %), followed by urgent (22, 2.8 %) and immediate (9, 1.1 %) referrals. Table 1 enumerates the frequency and percentage of the total referrals according to the specialty of referral and the referral type from each PHC.
The most frequently referred specialty was internal medicine with 163 (20.4 %) referrals, followed by obstetrics and gynecology (134, 16.8 %), orthopedics (104, 13 %), and general surgery (89, 11.1 %), and dermatology clinic (81, 10.1 %). All other specialties were less than 10 %. Most referrals were for diagnosis verification and management; others were general checkups, patient requests, or follow-ups. More details and explanations are shown in Figure 1.
Internal medicine was the most frequent referral, with 163 referrals. Results showed that 102 (62.6 %) were female, and 61 (37.4) were male. Most of the referrals were from Laban PHC with 88 cases (54 %), then from Tweeq Al-Qarbi PHC with 63 patients (38.7 %) and only 12 points (7.4 %) were from Al-Malaz PHC. Moreover, most of the referrals were elective, with 155 referrals (95.1 %) and 6 (3.7 %) and no urgent referrals.
Table 1: Data showing the frequency (percentage) of the total referrals according to the specialty of referral, showing the three centers and referral types
|
Specialty |
All |
Female |
Male |
Malaz |
Laban |
Tweeq |
Elective |
Immediate |
Urgent |
|
n (%) |
(n = 799) |
473 (59.2 %) |
326 (40.8 %) |
51 (6.4 %) |
385 (48.2 %) |
363 (45.4 %) |
768 (96.1 %) |
9 (1.1 %) |
22 (2.8 %) |
|
Internal Medicine |
163 (20.4 %) |
102 (21.6 %) |
61 (18.7 %) |
12 (23.5 %) |
88 (22.9 %) |
63 (17.4 %) |
155 (20.2%) |
2 (22.2 %) |
6 (27.3 %0 |
|
General Surgery |
89 (11.1 %) |
46 (9.7 %) |
43 (13.2) |
9 (17.6 %) |
43 (11.2 %) |
37 (10.2 %) |
84 (10.9 %) |
3 (33.3 %) |
2 (9.1 %) |
|
Ophthalmology Clinic |
64 (8 %) |
25 (5.3 %) |
39 (12 %) |
2 (3.9 %) |
45 (11.7 %) |
17 (4.7 %) |
64 (8.3 %) |
|
|
|
ENT |
62 (7.8 %) |
32 (6.8 %) |
30 (9.2 %) |
3 (5.9) |
41 (10.6 %) |
18 (5 %) |
61 (7.9 %) |
|
1 (4.5 %) |
|
Obstetrics & Gynecology |
134 (16.8 %) |
134 (28.3 %) |
0 (0 %) |
6 (11.8) |
39 (10.1 %) |
89 (24.5 %) |
125 (16.3 %) |
2 (22.2 %) |
7 (31.8 %) |
|
Orthopedics |
104 (13 %) |
52 (11 %) |
52 (16 %) |
12 (23.5) |
54 (14 %) |
38 (10.5 %) |
101 (13.2 %) |
|
3 (13.6 %) |
|
Pediatrics |
33 (4.1 %) |
16 (3.4 %) |
17 (5.2 %) |
3 (5.9 %) |
17 (4.4 %) |
13 (3.6 %) |
31 (4 %) |
|
2 (9.1 %) |
|
Derma Clinic |
81 (10.1 %) |
50 (10.6 %) |
31 (9.5 %) |
3 (5.9 %) |
38 (9.9 %) |
40 (11 %) |
81 (10.5 %) |
|
|
|
Urology Clinic |
37 (4.6 %) |
6 (1.3 %) |
31 (9.5 %) |
1 (2 %) |
20 (5.2 %) |
16 (4.4 %) |
34 (4.4 %) |
2 (22.2 %) |
1 (4.5 %) |
|
Obesity Clinic |
32 (4 %) |
10 (2.1 %) |
22 (6.7 %) |
0 (0 %) |
0 (0 %) |
32 (8.8 %) |
32 (4.2 %) |
|
|
ENT: ear, nose, and throat specialty
Discussion
Typically, PHC physicians are the leading practitioners who first provide definitive care to undifferentiated patients and take continuing responsibility for providing comprehensive care. A referral is a process of directing or redirecting the patient to the optimal level of care to provide complete care, usually from the lower to the greatest potential ones. The referral system must obtain diagnosis requests, confirmation, specialized medical treatment, surgical intervention, and laboratory tests.
In this study, the referral ratio of females to males was 60:40. When the referral for obstetrics and gynecology was excluded, the difference between male and female proportions became insignificant. In addition, the age ranged from months to 99 years in all three PHCCs, with no significant differences (p < 0.01) between these centers.
PHC physicians provide regular health care and should only refer exceptional cases for the following reasons [14,15]:
- To find better care with an expert opinion
- To avail advanced resources
- To obtain radiographic and laboratory work
- To receive inpatient services
- To reassure the patient or the patient's family of the absence of a severe disease
- To motivate the patient to adhere to medical advice
- To enhance patient's trust in their medical judgment
- No sufficient time to evaluate the patient thoroughly
A referral is associated with socioeconomic circumstances, which drive guidance and potentially life-threatening conditions [16], and a potential area for quality improvement [17]. In a PHCC, the effectiveness of the referral system suggests various ways of dealing with PHC physicians. Referrals might be reduced by providing professional training for the PHC physicians and might be improved by utilizing the referral guidelines of the World Health Organization [18].
In this study, 799 referrals were collected from different PHCCs to a tertiary care hospital, with a mean age of 38.8 years, including both males and females. Most referrals were elective (96.1 %), with internal medicine as the most commonly referred specialty (20.4 %). If all PHC physicians were well trained, we found no particular reason that internal medicine had the most referrals. In a previous study, patients were very keen with their physicians, and no relationship was found between specialty care and referrals [19]. However, internal medicine covers most diseases that PHC physicians should manage. If PHCCs have their interior medicine specialties or consultants, care provided to patients might be improved, and referrals could be reduced or not required. Thus, PHC physicians should be trained to deal with most internal medicine cases. Another reason for referring to internal medicine is the lack of radiologic machines in PHCCs. These tools play a significant role in helping physicians diagnose patients quickly and provide the needed management immediately.
Referral processes and their applicability should have specific measures to assess limited aspects of the referral process. Some referrals are generally deemed unnecessary but are considered substantial; one of these is dermatologic consultation [20]. However, the present study showed that dermatology was the fifth most referred specialty (Figure 1), showing the misinterpretation of the referral system. Moreover, PHC physicians make referrals probably because they want a second opinion for cases such as cancer. Therefore, to deliver better care to patients at PHCC, we need to establish specialized clinics for the most commonly referred specialties, such as internal medicine, obstetrics and gynecology, and orthopedics, and to have a referral back to the PHCC for continuity of care, given that most of the referred patients are not followed up after the referral.
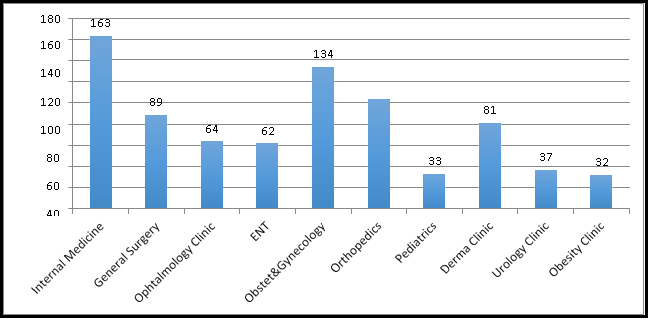
Figure 1: Number of referrals from primary health care centers to specific specialties at a tertiary care hospital
Conclusion
The most common referral was internal medicine referral. Unexpectedly, a dermatological referral was the fifth most common one, thereby considered substantial by many. The referral process should be revised with consideration of the less regarded referrals.
Most importantly, establishing specialized clinics for the most commonly referred specialties such as internal medicine, obstetrics and gynecology, and orthopedics and having a referral back to the PHC is essential to reduce the flow to secondary and tertiary hospitals.
Ethics approval and consent to participate
Ethical approval was granted from the institutional review board of King Saud Medical City (proposal reference H1RI-17-Dec20-01).
All methods in this study were performed by good clinical practice standards.
Competing interests: The authors declare that they have no conflict of interest.
Funding: None
Acknowledgments: The authors acknowledged all respondents to thank the research and innovation center for assisting and contributing to this project.
References
- Cervantes K, Salgado R, Choi M, Kalter HD (2003) Rapid assessment of referral care systems. Aguide for program managers. Edited by: Basics J. Basics, JSI, USAID.
- Al Ghamdi OM, AL-Malki BM, Eid Nahhas A, AL-Malki AD (2015) Rate of referral from primary health care to secondary health care among governmental hospitals in Taif governorate, KSA. International Journal of Medical Science and Public Health. 4(10): 1457-1463.
- Jarallah JS (1991) The quality of referral letters in two health centers in Riyadh. Annals of Saudi Medicine. 11(6): 658-62.
- Asuke S, Sabitu K, Ibrahim MS (2019) Pattern of referral before and after referral intervention among primary health centers in North-Western Nigeria. Archives of Medicine and Surgery. 4(1): 22-27.
- Legodi TL, Wolvaardt JE (2015) A blank page: feedback from first referral hospitals to primary health care clinics. South African Family Practice. 57(4): 282-285.
- Senitan M, Alhaiti A, Gillespie J (2018) “Ehalati”: Evaluation of the Referral System in Primary Health Care Centres in Saudi Arabia. International Journal of Integrated Care. 18 (s2): 326.
- Senitan M, Alhaiti AH, Gillespie J, Alotaibi BF, Lenon GB (2017) The referral system between primary and secondary health care in Saudi Arabia for patients with type 2 diabetes: A systematic review. Journal of Diabetes Research. 2017: 4183604.
- Al Asmri M, Almalki MJ, Fitzgerald G, Clark M (2020) The public health care system and primary care services in Saudi Arabia: a system in transition. Eastern Mediterranean Health Journal. 26(4): 468-476.
- Al Shamsi HS, Almutairi AG, Al Mashrafi SS (2018) Assessing the quality of the Saudi healthcare referral system: potential improvements implemented by other systems. Global Journal of Health Science. 10(11): 113.
- Kentish R, Jenkins P, Lask B (1987) Study of written communication between general practitioners and departments of child psychiatry. The Journal of the Royal College of General Practitioners. 37(297): 162-3.
- Epstein RM (1995) Communication between primary care Physicians and consultants. Archives of Family Medicine. 4(5): 403-9.
- Lee T, Pappius EM, Goldman L (1983) Impact of inter-physician communication on the effectiveness of medical consultations. The American Journal of Medicine. 74(1): 106-12.
- Al-Shehri AM, Thomas M, Al-Ghuli AM (1992) Use and misuse of emergency services at King Fahad Hospital, Riyad, Saudi Arabia. Saudi Medical Journal. 13(1): 21-4.
- Khoja TA, Al Shehri AM, Abdul Aziz AA, Aziz K. (1997) Patterns of referral from health centres to hospitals in Riyadh region. EMHJ-eastern Mediterranean Health Journal. 3(2): 236- 243.
- Donohoe MT, Kravitz RL, Wheeler DB, Chandra R, Chen A, et al. (1999) Reasons for outpatient referrals from generalists to specialists. Journal of General Internal Medicine. 14(5): 281-6.
- McBride D, Hardoon S, Walters K, Gilmour S, Raine R (2010) Explaining variation in referral from primary to secondary care: cohort study. BMJ. 341: c6267.
- Ringberg U, Fleten N, Deraas TS, Hasvold T, Førde O (2013) High referral rates to secondary care by general practitioners in Norway are associated with GPs’ gender and specialist qualifications in family medicine, a study of 4350 consultations. BMC Health Services Research. 13(1): 147.
- Hirsch O, Träger S, Bösner S, Ilhan M, Becker A, et al. (2012) Referral from primary to secondary care in Germany: developing a taxonomy based on cluster analysis. Scandinavian Journal of Public Health. 40(6): 571-8.
- Alberdi-Ordiozola JC, Sáenz-Bajo N (2006) Factors affecting primary care referrals to specialised care in the Community of Madrid. Atencion Primaria. 37(5): 253-7.
- Walia NS, Deb S (2004) Dermatology referrals in the hospital setting. Indian Journal of Dermatology Venereology and Leprology. 70(5): 285-7.