


Ghada Sahraoui1,2, Farah Sassi1*, Lamia Charfi1,2, Maroua Manai3, Aida Jlassi2, Hayet Douik1,2, Lamia Naija4, Khadija Meddeb5, Karima Mrad1,2, Raoudha Doghri1,2
1Pathology Department, Salah Azaiez Institute, Tunis, Tunisia
2Research Laboratory LR21SP01, Salah Azaiez Institute, Tunis, Tunisia
3Human Genetics Laboratory LR99ES10, University of medecine of Tunis, University of Tunis El Manar, Tunis, Tunisia
4Surgical Oncology Department, Salah Azaiez Institute, Tunis, Tunisia
5Medical Oncology Department, Salah Azaiez Institute, Tunis, Tunisia
*Corresponding Author: Farah Sassi, Pathology Department, Salah Azaiez Institute, Tunis, Tunisia. ORCID: 0000-0003-2078-6795
Abstract
Introduction: Endometrial carcinoma (EC) is an ever-growing gynecologic malignancy worldwide. The PD-1/PD-L1 immune checkpoints are among the critical players in immunosuppression in the tumor microenvironment. Currently, they are considered predictive markers for immunotherapy, particularly in EC.
This study aimed to determine PD-1 and PD-L1 expression in the tumor environment and their impact on prognosis.
Methods: A retrospective study was conducted in the Pathology Department of Saleh Azaiez Institute, involving 46 cases of EC over 10 years from January 2007 to December 2017. Clinicopathologic data were collected from medical records and pathology reports. Immunohistochemical analysis was performed on FFPE samples (the primary tumor) using an automaton (Leica Biosystems™).
Results & Discussion: Our series included 70% of postmenopausal women. Stage I (45.6%) and grade 1 (39.1%) were the most dominant. The superficial endometrial invasion was noticed in 67% of patients.
PD-L1 and PD-1 are expressed in 43% (26% in tumor-infiltrating lymphocytes and 17% in tumor cells) and 63% in tumor-infiltrating lymphocytes, respectively. PD-L1 was significantly associated with menopausal status and superficial myometrial invasion (p=0.001 and p=0.037, respectively). However, no association was found between PD-1 expression and prognostic features ofECs.
Our study indicated that EC has a heterogeneous immunogenic profile, which emphasizes the controversial role of PD-1/PD-L1 immune checkpoints in tumor progression.
Conclusion: PD-1/PD-L1 expression in EC is remarkable, without relevant association with prognostic elements. Future research on a more extensive series may be helpful to detect clearly the role of these biomarkers in tumor progression.
Keywords: PD-L1, PD-1, Immunotherapy, Biomarkers, Immunohistochemistry, Endometrial cancer
Introduction
Endometrial cancer (EC) is the most common gynecologic cancer in high-income countries and the second most common cancer after cervical cancer in low-income countries [1,2]. Identifying new prognostic and therapeutic biomarkers is necessary to stratify patients according to their tumor biological characteristics for targeted treatment therapies [3]. Immune checkpoint inhibitors like anti-programmed death protein 1 (PD-1) and its ligand (PD-L1) have been an effective therapeutic option in oncology in recent years and have been well studied in various cancers (lung cancer and melanoma.). In ECs, the FDA approved pembrolizumab (PD-1-inhibitor) for treating microsatellite unstable recurrent and metastatic ECs [4]. In primary ECs, expression patterns of PD-L1 and PD-1 have been little studied [5]. This study aimed to investigate the PD-L1/PD-1 expression in tumor and immune cells in ECs and to analyze its prognostic value.
Methods
Patient samples
We conducted a retrospective study that included 46 cases of ECs. All patients diagnosed on surgical specimens or biopsy curettages were collected at the Pathology Department of Salah Azaiez Institute between 2007 and 2017. Claims that paraffine blocks were not usable or not available were excluded from the study. All patients were staged according to FIGO 2009 criteria. Clinical (age, parity, menopausal status, medical history) and pathological (grade, the degree of myometrial invasion, vascular emboli, FIGO stage, local recurrence, distant metastasis, and survival outcomes) were obtained from clinical and pathological records. The histological diagnosis followed the classification of Female Genital Tumors by World Health Organization (WHO 2020) [6].
Tissue microarray (TMA)
Tissue microarrays (TMAs) from Formalin-Fixed Paraffin-Embedded (FFPE)were constructed. The area with the highest tumor grade was identified on hematoxylin and eosin-stained slides. Two tissue cores of 0.6 mm diameter from each case were punched out of a tissue array device and mounted in a paraffin block.
Immunohistochemistry (IHC)
TMA slides (4 μm) were cut and dewaxed with xylene and rehydrated in ethanol, and antigen retrieval was performed by microwaving, pH 6 for PD-L1 and pH 9 for PD-1. Following peroxidase block, the TMAs were incubated for 30 min at room temperature with rabbit monoclonal antibody to PD-L1 (22C3,1:50, LEICA) and rabbit monoclonal antibody to PD-1 (IHC001, 1:100-1:400, LEICA) followed by 30 min of incubation with secondary HRP-conjugated anti-rabbit antibody and 8 min with DAB-chromogen (EnVision detection system, Dako). Sections of tonsil samples were used as positive controls.
Analysis of PD-1 and PD-L1 Expression
Assessment PD-L1 expression was evaluated by a semi-quantitative method according to the intensity of cytoplasmic and/or membranous positivity: 0 (no staining), 1+ (mild staining), 2+ (moderate staining) or 3+ (intense staining) [7]. Tumor cells and tumor-associated immune cells, including tumor-infiltrating lymphocytes (TILs) and peritumoral inflammatory cells (lymphocytes and macrophages in the stroma immediately adjacent to the tumor epithelium) at tumor edges were considered as positive staining using a cut-off score ≥1%[8].PD- 1 expression was evaluated inTILs. The selected area of the tonsil specimen served as positive control tissue.
Statistical analysis
Statistical analyses were performed using SPSS 26.0. The χ2 and Fisher's tests were used to determine associations between PD-1 and PD-L1 expression and clinicopathological features (age, menopausal status, metastasis, FIGO stage, histological grade, and myometrial invasion) in ECs. P-values < 0.05 were considered significant.
Results
Clinicopathological characteristics
The patient's age ranged from 34 to 87 years, with a mean of 59± 10.9 years. Among the cases, 24 (52.2 %) of 46 were more than 60 years old. Thirty-one (67.4 %) patients were menopausal, and 4 (8.7 %) were peri-menopausal. ECs were low-grade (grade 1) in 18 (39.1 %). Considering data on clinical staging, 60.9 % were stage I-II, 28.3 % stage III, and 4.3 % stage IV. Invasion of the myometrium was observed in 42 cases (91 %). Invasion of more than half of the myometrium was observed in 15 cases (33 %). Extension to the cervix was found in 4 cases (8.7 %). Vascular emboli were observed in 4 cases (8.7 %). Recurrence was observed in 11 patients (24 %). The evolution was marked by distant metastasis in 7 patients (15.2 %). The metastases were in the liver in 5 cases (11%) and in the lungs in 3 cases (6.5 %). The clinicopathologic data of the patients are shown in Table 1.
Correlation of PD-L1 and PD-1 expression with clinicopathological features in ECs
PD-L1 expression in tumor cells and tumor-associated immune cells
PD-L1 was expressed in 8 cases (17 %), with a percentage of stained tumor cells ranging from 1 to 50 %. The staining was of mild intensity in 5 patients (62.5 %) and moderate intensity in 3 patients (37.5 %). PD-L1 was expressed in lymphocytes in 12 cases (26.1 %), with a percentage of stained cells ranging from 1 % to 5 % (Figure 1 and Table 2).
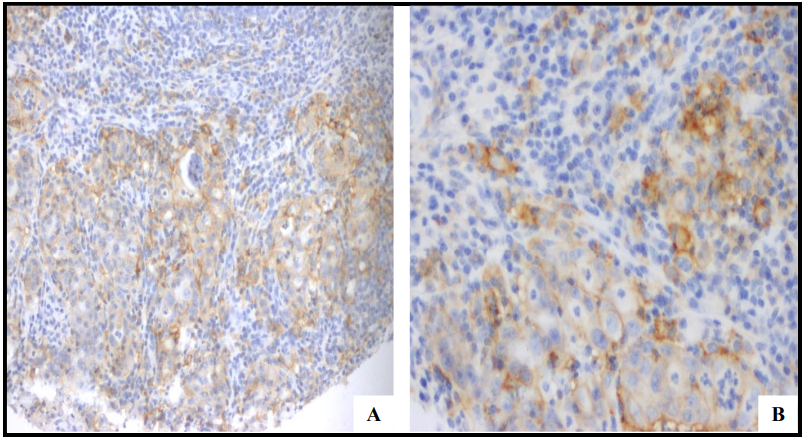
Figure 1: Immunohistochemical staining for PD-L1 in endometrial cancer:
A/ Membrane staining of 30 % of tumor cells (mild to moderate intensity) x200
B/ Membrane staining of 5 % of intratumoral lymphocytes (mild to moderate intensity) x400
Table 2: Staining intensity of PD-L1 expression in tumor cells and tumor associated lymphocytes in endometrial carcinomas
|
|
PD-L1 + n (%) |
|
|
Intensity |
Tumor cells |
Tumor associated lymphocytes |
|
< 1 % |
38 (82,6) |
34 (73,9) |
|
1-30 % |
6 (13,1) |
12 (26,1) |
|
> 30 % |
2 (4,3) |
0 (0) |
Correlation of PD-L1 expression with clinicopathological features
PD-L1 expression in tumor cells and clinicopathological features
The PD-L1+ phenotype in tumor cells was more observed in patients older than 60 years (62.5 % versus 37.2 %), with no significant association. A significant association was found between PD-L1+ tumor cells and menopausal status (p=0.001), myometrial invasion < 50 % (p=0.037). PD-L1+ ECs were predominantly stage I and low grade (62.5 %) with no significant association (Table 3).
Table 3: Association of PD-L1 expression in tumor cells with prognostic histopathological parameters in endometrial carcinomas
|
Clinicopathologic characteristics |
PD-L1 + expression in tumor cells n (%) |
p-value |
|
FIGO stage |
|
0,873 |
|
I |
5 (62,5) |
|
|
II |
1 (12,5) |
|
|
III |
2 (25) |
|
|
IV |
0 (0) |
|
|
Grade |
|
0,855 |
|
G1 |
5 (62,5) |
|
|
G2 |
2 (25) |
|
|
G3 |
1 (12,5) |
|
|
Myometrial invasion |
|
0,037 |
|
≥ 50 % |
3 (37,5) |
|
|
< 50 % |
5 (62,5) |
|
|
Distant metastasis |
|
0,436 |
|
Yes |
0 (0) |
|
|
No |
7 (87,5) |
|
PD-L1 expression in tumor-infiltrating lymphocytes and clinicopathological features
PD-L1+ tumor-infiltrating lymphocytes were more observed in patients younger than 60 (58 % versus 42 %) with no significant association. A significant association was found between PD-L1+ lymphocytes and menopausal status (p=0.014). No significant association of PD-L1+ lymphocyte status with histological prognostic parameters was demonstrated (Table 4).
Table 4: Association of PD-L1 expression in tumor associated immune cells with prognostic histopathological parameters in endometrial carcinomas
|
Clinicopathologic characteristics |
PD-L1 expression in tumor associated immune cells n (%) |
p-value |
|
FIGO stage |
|
0,726 |
|
I |
7 (58,3) |
|
|
II |
1 (8,3) |
|
|
III |
4 (33,3) |
|
|
IV |
0 (0) |
|
|
Grade |
|
0,930 |
|
G1 |
5 (41,6) |
|
|
G2 |
2 (16,6) |
|
|
G3 |
5 (41,6) |
|
|
Myometrial invasion |
|
0,238 |
|
≥ 50 % |
3 (25) |
|
|
< 50 % |
9 (75) |
|
|
Distant metastasis |
|
0,558 |
|
Yes |
0 (0) |
|
|
No |
6 (50) |
|
PD-1 expression in tumor-associated immune cells
PD-1 was expressed by lymphocytes in 29 cases (63 %), with a percentage of stained cells ranging from 1 to 30 % (Figure 2). Co-expression of PD-1 and PD-L1 in immune cells was detected in 11 cases (24 %). In addition, PD-1 expression in lymphocytes and PD- L1 expression in tumor cells were noted in 7 cases (15.21 %).
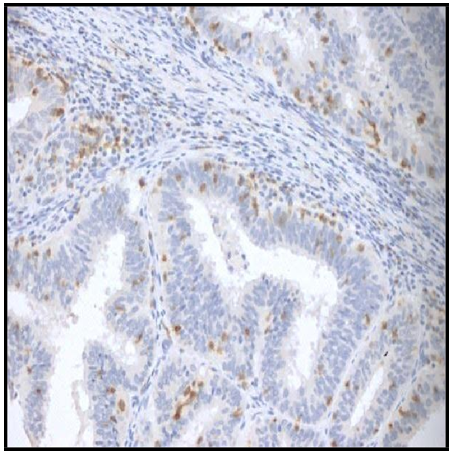
Figure 2: Immunohistochemical staining for PD-1 in immune cells, strong cytoplasmic and membranous staining x400
Correlation of PD-1 expression with clinicopathological features
No statistical association was detected between clinicopathological and prognostic variables and the PD-1+ lymphocytes (Table 5).
Table 5: Association of PD-1 expression in tumor associated immune cells with prognostic histopathological parameters in endometrial carcinomas
|
Clinicopathologic characteristics |
PD-1+ expression n (%) |
p-value |
|
Age |
|
0,248 |
|
≥ 60 ans |
15 (51,7) |
|
|
≤ 60 ans |
14 (48,3) |
|
|
Menopausal status |
|
0,072 |
|
Oui |
21 (72,4) |
|
|
Non |
8 (27,6) |
|
|
FIGO stage |
|
0,254 |
|
I |
16 (55,2) |
|
|
II |
3 (10,3) |
|
|
III |
7 (24,1) |
|
|
IV |
2 (6,9) |
|
|
Grade |
|
0,293 |
|
G1 |
12 (41,4) |
|
|
G2 |
7 (24,1) |
|
|
G3 |
10 (34,5) |
|
|
Myometrial invasion |
|
0,153 |
|
≥ 50 % |
10 (34,5) |
|
|
< 50 % |
19 (64,5) |
|
|
Distant metastasis |
|
0,295 |
|
Yes |
4 (13,8) |
|
|
No |
25 (86,2) |
|
Discussion
Recently, there has been a rising interest in immunotherapy inpatient treatment. Therapeutics are being developed against the potential targets PD-1 and PD-L1.PD-L1 expression is elevated in EC compared to non-malignant endometrial tissue, although the prognostic value is currently not entirely understood [9].
The literature revealed significant variability in PD-L1 favorable rates (from 0.9 to 44.3 %) and showed various PD-L1 expression profiles among molecular subclasses, histologic subtypes, and tumor stages [3,10,11]. In a recent study, PD-L1 expression in tumor cells was observed in 15 % of type II ECs [7]. In contrast, a study reported that 70 % of ECs (type I and II) expressed PD-L1 without specifying the cut-off [12]. The diversity of immunohistochemical techniques for PD-L1 testing or the interpretation algorithm explains the results' divergence. This heterogeneity gives a different implication of PD- 1/PD-L1 therapy. Hence there is a need for standardization and validation of PD-L1 immunohistochemical study to increase the reliability of this antibody [11,13]. Our study noted PD-L1 expression in tumor cells in only 17 % of cases.
Our study noted PD-L1 expression in intra-tumoral lymphocytes in 26 % of cases. In this context, a large study including 700 patients showed that PD-L1 was positive in about 59 % of cases (including endometrioid adenocarcinomas and type II carcinomas) [1]. Furthermore, it has been reported that PD-L1 is more frequently expressed in intra-tumoral lymphocytes in ECs with microsatellite instability [14]. Nearly 65 % of ECs are PD-1+ [15]. Moreover, PD- 1 expression was significantly associated with type I ECs (p=0.001) [16]. Similarly, in this study, PD-1 expression in intra-tumoral lymphocytes was noted in 63 % of cases.
This study demonstrated a positive correlation between PD-L1 expression and menopausal status, which is in accordance with the literature. This expression is significantly less frequent before menopause [11,17]. The variation of PD-L1 words according to hormonal status can be explained by the absence of cyclic hormonal variations after menopause. Thus, the tumor microenvironment and the immune response in the endometrium would be influenced by hormonal fluctuations [17].
The prognostic value of PD-L1 status in ECs remains controversial. A significant association of PD-L1 with deep myometrial invasion (> 50 %) is reported [16,18]. In contrast, a study demonstrated that PD- L1 expression in tumor cells was associated with invasion of less than 50 % of the myometrial thickness (p=0.0037) [12]. This study found a significant association between PD-L1 expression in tumor cells and invasion of less than half of the myometrium (p=0.037). On the other hand, according to some authors, the expression of PD-L1 in intra- tumoral lymphocytes is significantly associated with high-grade and advanced endometrial carcinomas [5,7]. However, no significant association between PD-L1 expression and stage or histological grade was found in this report. PD-L1 expression in intra-tumoral lymphocytes is significantly associated with POLE ultramutantECs and microsatellite instability [16].
According to a recent meta-analysis, PD-L1 status did not influence overall survival or disease progression in endometrial carcinomas [3]. Similarly, Oliviero Marinelli et al. noted that PD-L1 expression by tumor cells was not correlated to survival rates [16]. In contrast, a study demonstrated that PD-L1 expression by tumor cells was associated with better survival, whereas PD-L1 expression by immune cells was significantly associated with worse prognosis and advanced FIGO stage [12]. The data in the literature are divergent concerning the prognostic value of PD-1 status. Our study found no correlation between PD-1 rate and clinicopathological parameters.
Most studies have demonstrated the absence of prognostic impact of PD-1+ status in ECs.
It did not correlate with histological prognostic factors or survival rates [1,7]. However, according to Jesup K et al., PD-1+ status was associated with better overall survival [15]. In another study, PD-1 expression was associated with non-endometrioid type II carcinoma [5]. Other authors reported a significant association between PD-1 status and microsatellite instability (MSI) in ECs [16].
Recent research in advanced melanoma suggests a classification of the tumor microenvironment based on TILs and the degree of PD-L1 expression [12,15]. According to the same source, the PD-L1+ TILs responded favorably to immune checkpoint blockade therapy during clinical trials [12]. These data highlight emerging issues in oncology, such as "personalized medicine" centered on biological markers.
The retrospective monocentric study design with a relatively small sample size of patients is the major limitation of this study. More extensive trials need to be conducted to assess the general applicability of PD-1/PD-L1 inhibitors in EC therapy.
The PD-L1/PD-1 profile may be of interest as a predictor of response to immunotherapy by immune checkpoint blockade. This hypothesis requires better evaluation of biomarkers in the subtypes of the molecular classification of ECs to give more accurate inferences.
Finally, in the absence of a proven solid association between PD- L1/PD-1 profile and disease prognosis, these biological checkpoints can be exploited as predictive markers of treatment response.
These factors can be used to categorize candidates who will respond best to immunotherapy or who will be selected for additional, expensive molecular research.
Conclusion
This study showed a higher expression of PD-L1 in tumor-infiltrating lymphocytes than in tumor cells. PD-1 was expressed in 63 % of cases. PD-L1 was significantly associated with menopausal status and myometrial invasion. Less than 50 %. No association was found between PD-1 expression and prognostic histological features of ECs. This study may be an opening point for exploiting the PD-1/PD-L1 axis in treating ECs.
Declarations
Sources of funding: This research did not receive any specific grant from the public, commercial, or not-for-profit funding agencies.
Data availability statement:ss Data will be made available on request.
Credit authorship contribution statement: All the authors read and approved the final version of the manuscript.
Farah Sassi (MD): conception, acquisition of data, literature research, and preparing the manuscript
Ghada Sahraoui (MD): acquisition of clinical data, preparing and revising the manuscript
Lamia Charfi (MD): Supervision, prepare and revise the manuscript
Maroua Manai (MD): Analyzed and interpreted the data
Aida Jlassi (MD): Analyzed and interpreted the data
Hayet Douik (MD): Analyzed and interpreted the data
Lamia Naija (MD): Acquisition of clinical data
Khadija Meddeb (MD): Acquisition of clinical data
Karima Mrad (MD): Manuscript editing, Revising the manuscript critically
Raoudha Doghri (MD): Acquisition of data, manuscript editing, final approval of the version to be published
Declaration of competing interest: The authors report no declarations of interest.
References
- Engerud H, Berg HF, Myrvold M, Halle MK, Bjorge L, et al. (2020) High degree of heterogeneity of PD-L1 and PD-1 from primary to metastatic endometrial cancer. Gynecol Oncol. 157(1): 260–267.
- Doghri R, Yahyaoui Y, Gabsi A, Driss M, Boujelbene N, et al. (2018) Endometrial carcinoma: An histopathological and histoprognotic study about 62 patients in a center in the Tunisian north. Ann Pathol. 38(2): 85–91.
- Lu L, Li Y, Luo R, Xu J, Feng J, et al. (2020) Prognostic and Clinicopathological Role of PD-L1 in Endometrial Cancer: A Meta-Analysis. Front Oncol. 10: 632.
- Di Tucci C, Capone C, Galati G, Iacobelli V, Schiavi MC, et al. (2019) Immunotherapy in endometrial cancer: new scenarios on the horizon. J Gynecol Oncol. 30(3): e46.
- Mo Z, Liu J, Zhang Q, Chen Z, Mei J, et al. (2016) Expression of PD-1, PD-L1 and PD-L2 is associated with differentiation status and histological type of endometrial cancer. Oncol Lett. 12(2): 944–950.
- Höhn AK, Brambs CE, Hiller GGR, May D, Schmoeckel E, et al. (2021) 2020 WHO Classification of Female Genital Tumors. Geburtshilfe Frauenheilkd. 81(10): 1145–1153.
- Kucukgoz Gulec U, Kilic Bagir E, Paydas S, Guzel AB, Gumurdulu D, et al. (2019) Programmed death-1 (PD-1) and programmed death-ligand 1 (PD-L1) expressions in type 2 endometrial cancer. Arch Gynecol Obstet. 300(2): 377–382.
- Hecking T, Thiesler T, Halbe J, Otten L, Recker F, et al. (2022) Programmed Cell Death Ligand-1 (PDL-1) Correlates With Tumor Infiltration by Immune Cells and Represents a Promising Target for Immunotherapy in Endometrial Cancer. Anticancer Research. 42(3): 1367–1376.
- Sungu N, Yildirim M, Desdicioglu R, Başaran Aydoğdu Ö, et al. (2019) Expression of Immunomodulatory Molecules PD-1, PD- L1, and PD-L2, and their Relationship With Clinicopathologic Characteristics in Endometrial Cancer. Int J GynecolPathol. 38(5): 404–413.
- Mo Z, Liu J, Zhang Q, Chen Z, Mei J, et al. (2016) Expression of PD-1, PD-L1 and PD-L2 is associated with differentiation status and histological type of endometrial cancer. Oncol Lett. 12(2): 944-950.
- Marinelli O, Annibali D, Aguzzi C, Tuyaerts S, Amant F, et al. (2019) The Controversial Role of PD-1 and Its Ligands in Gynecological Malignancies. Front Oncol. 9: 1073.
- Zhang S, Minaguchi T, Xu C, Qi N, Itagaki H, et al. (2020) PD- L1 and CD4 are independent prognostic factors for overall survival in endometrial carcinomas. BMC Cancer. 20: 127.
- Jubel JM, Barbati ZR, Burger C, Wirtz DC, Schildberg FA (2020) The Role of PD-1 in Acute and Chronic Infection. Front Immunol. 11: 487.
- Howitt BE, Shukla SA, Sholl LM, Ritterhouse LL, Watkins JC, et al. (2015) Association of Polymerase e-Mutated and Microsatellite-Instable Endometrial Cancers with Neoantigen Load, Number of Tumor-Infiltrating Lymphocytes, and Expression of PD-1 and PD-L1. JAMA Oncol. 1(9): 1319–23.
- Kim J, Kim S, Lee HS, Yang W, Cho H, et al. (2018) Prognostic implication of programmed cell death 1 protein and its ligand expressions in endometrial cancer. Gynecol Oncol. 149(2): 381– 387.
- Nobari N, Niknejad N, Poorolajal J, Vaezi M, Nili F, et al. (2020) Clinicopathologic Features and Prognostic Role of CD3, CD8, and PD-1 positive Tumor-Infiltrating Lymphocytes and the Association with COX-2 Overexpression in Endometrial Carcinoma. Int J Cancer Manag. 13(4): e99210.
- Shen Z, Rodriguez-Garcia M, Patel MV, Barr FD, Wira CR (2016) Menopausal status influences the expression of programmed death (PD)-1 and its ligand PD-L1 on immune cells from the human female reproductive tract. Am J Reprod Immunol. 76(2): 118–25.
- Evsei A, Birceanu-Corobea A, Ghita M, Copca N, Sajin M (2021) Tumour microenvironment and PD-L1 expression in endometrial carcinoma. Arch Balk Med Union. 56(1): 8-15.