


Samar Shaban Abdelazim Mohamed1, Hanan Elzeblawy Hassan1*, Amel Ahmed Hassan Omran2, Elham Abozied Ramadan2
1Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt
2Obstetrics Gynecological Nursing, Faculty of Nursing Benha University
*Corresponding Author: Hanan Elzeblawy Hassan, Maternal and Newborn Health Nursing, Faculty of Nursing, Beni-Suef University, Egypt.
Abstract
Background: Urinary incontinence, in whichever forms, intensively affects the QOL of women. The symptoms are perceived as a poor health which ultimately affects the holistic well-being.
Aim of the study: Assess correlation urinary incontinence among elderly women and their physical condition.
Subject and Methods: A Purposive sample was used from the above-mentioned setting. Total sample was 100 women who attended to gynecological and urological outpatient clinics at Beni-Suef University Hospital.
Tools: (1): A structured interviewing questionnaire sheet. It was consisting of two parts: The first part: included personal characteristics data of the study women. The second part: included obstetrics history. (2): The International Consultation on Incontinence Modular Questionnaire ICIQ- SF.
Results: the mean age of the studied sample was 54.23±2.87, and 71% were from rural areas, 66% delivered spontaneous vaginally, and 25% delivered vaginally with episiotomy. It indicates that 45% of the studied women reported urine leakage several times a day, while 30% leak two or three times a week.
Conclusion: Urinary incontinence had positive effect on physical conditions “daily activities as shopping, cooking, cleaning, and practicing any type of sport”.
Recommendations: Application of an education program regarding healthful practices to avoid urinary incontinence among elderly women
Keywords: Urinary Incontinence, Physical Condition
Introduction
Elder people may have a combination of detrusor over activity on filling and poor contractility during voiding, a condition termed detrusor hyperactivity with impaired contractility (DHIC). In such cases, the bladder contraction does not empty. The bladder fully, leaving a large post-void residual (which otherwise is not explained by bladder outlet obstruction). Symptoms include leakage with urgency, leakage with increases in abdominal pressure, dribbling, frequency, and nocturnal similar to other LUT conditions such as stress UI and obstruction, for which DHIC easily can be mistaken people [1].
In women, mucosal thinning and lack of proteoglycans reduce urethral wall apposition and may contribute to retrograde movement of perineal bacteria into the bladder causing urinary tract infections. These mucosal changes may extend up to the bladder trigon, causing irritation of sensory afferent nerves, and possibly triggering involuntary detrusor contractions. The change in volume, consistency, and vascularity of the sub mucosa also lessens resting urethral compression [2-4].
The submuscosal venous plexus in the proximal urethra loses its corkscrew shape, the number and volume of arterial vessels decrease, and vascular pulsations lessen. All of these changes contribute to the observed decrease in urethral closure pressure in older women. All of these changes contribute to the observed decrease in urethral closure pressure in older women [2].
The prevalence of age-related changes in the vagina can vary with hormonal status, coexistent vascular disease, and the continuation or lack of sexual activity. The postmenopausal decrease in estrogen plays a part in many age-associated vaginal changes. Estrogen is trophic for much of the LUT track in women, with estrogen receptors found in the vagina, vestibule, distal urethra, bladder trigon, pelvic muscles, and ligament [5].
Following menopause, the vaginal epithelium loses the majority of its superficial and intermediate layers. Mucosal thinning may be associated with inflammation, evident as erythema, friability, and erosions. This may be responsible for irritative LUTS in many elderly women In addition, there is loss of epithelial glycogen and lubrication, and mucosal pH increases from 4.5-5.5 to 7.0- 7.4 [5]
These changes can lead to loss of normal adherent flora (lactobacillus), and colonization with pathogenic organisms such as E coli and enterococci.
This in turn may result in recur- rent symptomatic urinary tract infections and some associated LUTS. Vaginal blood flow, which is important for mucosal integrity and sub mucosal fullness, decreases with age. The combined epithelial and stromal changes are associated with vaginal wall thinning and flattening of rugae [6].
Aim of the study
1. Assess sings & symptoms of urinary incontinence among elderly women according to ICIQ-SF scale.
2. Assess correlation urinary incontinence among elderly women and their physical condition
Research questions
1. What about sings & symptoms of urinary incontinence among elderly women according to ICIQ-SF scale?
2. Is their correlation urinary incontinence among elderly women and their physical condition?
Subject And Methods
Study Setting and Sampling:
A Purposive sample was used from the above mentioned setting. Total sample was 100 women who attended to gynecological and urological outpatient clinics at Beni-Suef University Hospital.
Tools of data collection:
Tools that were used for data collection:
Tool I: A structured interviewing questionnaire sheet was developed by the researcher in the Arabic language based on a review of recent literatures, under guidance of supervisors. It was consisting of two parts:
The first part: included personal characteristics data of the study women such as (age, height, weight, body mass index "BMI" education level, occupation, residence, marital status).
Second part: Obstetrics history such as (number of gravidity, parity, and abortion, mode of deliveries, any complications during pregnancy, labor and post-partum, mode of delivery, weight of baby at birth and duration between pregnancy).
Tool II: The International Consultation on Incontinence Modular Questionnaire ICIQ-SF: (sponsored by the World Health Organization (WHO) and organized by the International Consultation on Urological Diseases (ICUD, 1998): The ICIQ is a self-reported survey and screening tool for evaluating the frequency, severity of urinary incontinence. It consisted of 4 main items of 6 total ask for rating of symptoms in the past 4 weeks. Take sum score of items 3, 4, 5 (items 1 and 2 are demographic) for the actual score. The final item is a self-diagnostic item that is un-scored. The ICIQ-UI Short form provides a score ranging from 0-21; with a higher score indicating greater severity of symptoms; this assessment done before and after intervention.
Scoring system of The ICIQ-UI:
1. The total score is considered mild when <25% <10points).
2. Consider moderate when 25-50 % (10-15 points).
3. Consider sever when >50% (>15 points).
Statistical Design:
The collected data was revised, coded, tabulated and introduced to a computer using statistical package for social sciences (IBM SPSS.25.0). Data was presented and suitable analysis was done according to the type of data obtained for each parameter.
Results
Table (1): Reveals the distribution of studied sample according to personal characteristics. It shows that the mean age of the studied sample was 54.23±2.87, and 71% were from rural areas. Also, 30% of them were having primary educated and (87%) were married.
Table (2): Illustrates that 66% of the studied women were delivered spontaneous vaginally, while about 29% delivered by cesarean section, and 25% delivered vaginally with episiotomy. Regarding complications during pregnancy, the table reveals that 78% of the studied sample complained from untreated urinary tract & gestational diabetes (30% & 19%, respectively).
Table (3): displays the distribution of studied sample according to the International Consultation on Incontinence Modular Questionnaire (ICIQ-SF). It indicates that 45% of the studied women reported urine leakage several times a day, while 30% leak two or three times a week. Moreover, 61% of them reported that they leak small amount (under wear or pad is damp) of urine, while 32% leak moderate amount (under wear or pad is wet). In addition, all of them (100%) leak during cough or sneeze, while 24% leak before getting to the toilet.
Figure (1): Clarifies the distribution of studied sample according to their physical condition. It reveals that 43% of the studied women slightly practicing daily activities as shopping, cooking, cleaning. Moreover, 42% of the studied women were moderately practicing any type of sport. In addition, 43% of the studied women were moderately wearing any kind of clothes.
Table 1: Distribution of studied sample according to personal characteristics (n=100).
|
Personal Characteristics |
No |
% |
|
Age (in years) |
||
|
Mean ±SD 54.23±2.87 |
||
|
Residence |
||
|
Rural |
71 |
71. 0 |
|
Urban |
29 |
29.0 |
|
Education |
||
|
Illiterate |
49 |
49.0 |
|
Primary education |
30 |
30.0 |
|
Secondary education |
18 |
18.0 |
|
University education |
3 |
3.0 |
|
Marital status |
||
|
Married |
87 |
87.0 |
|
widower |
13 |
13.0 |
Table 2: Distribution of studied sample according to obstetrics history (n=100)
|
Obstetrics history |
No |
% |
|
*Type of delivery |
||
|
Spontaneous vaginal deliveries |
66 |
66.0 |
|
Vaginal deliveries with episiotomy |
25 |
25.0 |
|
Caesarean section |
29 |
29.0 |
|
Instrumental deliveries |
1 |
1.0 |
|
Duration between pregnancy |
||
|
Usually between 1 - 2 year |
4 |
4.0 |
|
Usually between 2- 3 years |
51 |
51.0 |
|
More than 3 years |
16 |
16.0 |
|
Not regular intervals |
29 |
29.0 |
|
*Complication during pregnancy |
||
|
No complications |
40 |
40.0 |
|
Antepartum hemorrhage |
15 |
15.0 |
|
Gestational Diabetes |
19 |
19.0 |
|
Pregnancy Induced Hypertension |
7 |
7.0 |
|
Untreated urinary tract infection |
30 |
30.0 |
|
Anemia |
7 |
7.0 |
*results not mutually exclusive
Table 3: Distribution of studied sample according to their ICIQ-SF scale (n=100)
|
ICIQ-SF scale |
No |
% |
|
Frequency of urine leakage |
||
|
About once a week or less often |
20 |
20.0 |
|
Two or three times a week |
30 |
30.0 |
|
About once a day |
5 |
5.0 |
|
Several times a day |
45 |
45.0 |
|
The amount of urine leakage |
||
|
A small amount (under wear or pad is damp) |
61 |
61.0 |
|
A moderate amount (under wear or pad is wet) |
32 |
32.0 |
|
A large amount (under wear or pad is very wet |
7 |
7.0 |
|
*Time of urine leakage |
||
|
Leaks before getting to the toilet |
24 |
24.0 |
|
Leaks during cough or sneeze |
100 |
100.0 |
|
Leaks during sleeping |
2 |
2.0 |
*results not mutually exclusive
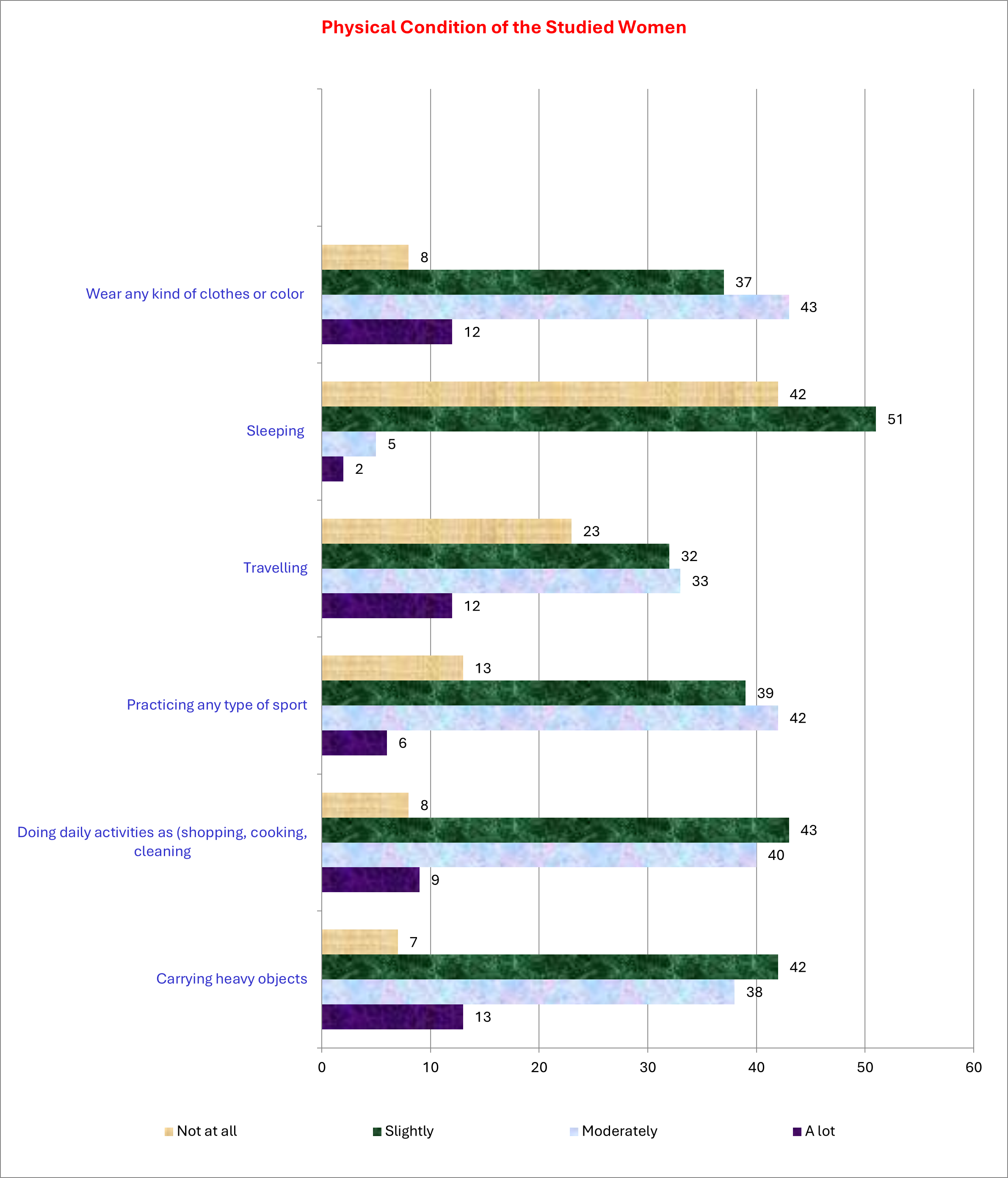
Figure 1: Distribution of studied sample according to their physical condition (n=100)
Discussion
Older women have many problems that affect their health, special problems with incontinence because of many changes may occur in the lower urinary tract due to aging, physical limitation and the environments in which they live [7].
Stress urinary incontinence results from failure of the sphincter mechanism to maintain outlet closure during bladder filling and increased intra-abdominal pressure during sneezing, coughing, running, laughing, or exertion greater physical effort [8].
In light of the high prevalence and the physical consequences of UI in menopausal women, it is necessary to determine an effective treatment for this problem. The International Continence Society recommends conservative treatment as the first line of treatment for incontinent women with a focus on increasing strength and correcting activating patterns of the pelvic floor muscles [9]
The results of the current study clarify that 43% of the studied women slightly practiced daily activities such as shopping, cooking, and cleaning. Moreover, 42% of the learned women were moderately practicing any type of sport. In addition, 43% of the studied women were moderately wearing any kind of clothes. This is in line with FeldeG et al. (2020), who reported that restrictions in physical activity, relationships, feelings of helplessness, increased risk of urinary tract infections (UTIs), pressure ulcers, falls, and fractures, all of which may lead to functional impairment and decline in overall health status (10). The restricted activities not only interfere with interpersonal relationships, but also it can damage self-esteem as a result of the shame and embarrassment some older adults feel, and those afflicted women health and quality of life [10]. So, this study conducted to examine the effect of urinary incontinence on physical conditions among elderly women.
The effect of age on pelvic floor structure and function is difficult to separate from the effects of hormonal status and parity. Evidence of denervation and changes in striated muscle fiber number, type, and diameter have been found in asymptomatic and nulliparous women. Constipation may contribute to pelvic floor dysfunction in older women. Total collagen content in pelvic muscle and fascia declines with age, with increased cross- linking and decreased elasticity, but this association does not imply a direct causative effect of “ageing.” [11].
The results of the current study show that the mean age of the studied sample was 54.23±2.87. This may explain the causes of incontinence. Age-related changes in these neurotransmitters, their receptors, or the cellular events they stimulate may be related to UI development in older people. Similarly, age-related changes in immune function may predispose older people to bacteriuria and recurrent urinary tract infections, which may be related to UI [6].
Conclusion:
Urinary incontinence had positive effect on physical conditions “daily activities as shopping, cooking, cleaning, and practicing any type of sport”.
Recommendations:
Application of an education program regarding healthful practices; to avoid urinary incontinence among elderly women.
References
- Kopańska M, Torices S, Czech J, Koziara W, Toborek M, et al. (2020) Urinary incontinence in women: biofeedback as an innovative treatment method. Therapeutic Advances in Urology. 123(34): 123-150.
- Cardoso AMB, Lima C, Ferreira CWS (2018) Prevalence of urinary incontinence in high impact sports athletes and their association with knowledge, attitude and practice about this dysfunction. Eur J Sport Sci. 18(10): 1405–1412.
- Hassan HE (2020) Kegels Exercises: A crucial issue during woman’s lifespan. American Research Journal of Public Health. 3(1): 1-5.
- Mohamed S, Omran A, Hassan H, Abo zied E (2023) Effect of Deep Breathing and Kegel Exercises on Stress Urinary Incontinence among Elderly Women. Benha Journal of Applied Sciences. 8(4): 81-89.
- Dos Santos KM, Da Roza T, Tonon da Luz SC, Hort JP, Kruger JM, et al. (2019) Quantification of urinary loss in nulliparous athletes during 1 hour of sports training. PM R. 11(5): 495–502.
- Aoki Y, Brown HW, Brubaker L, Cornu JN, Daly JO, et al. (2017) Urinary incontinence in women. Nat Rev Dis Primers. 3: 17042.
- El Badawy RES, Ali SA, Abo El-Seoud AR, Abd Allah ES (2019) Health Education Intervention for Controlling of Stress Urinary Incontinence among Elderly Women at Zagazig City. Zagazig Nursing Journal. 9(2): 49-65.
- Wang SP, Zhang YJ, Zhang HL, Lu S (2019) Investigate of prevalence rate and influencing factors of stress urinary incontinence among menopausal women in Wuhan [Original in Chinese]. Chinese Journal of Family Plan Gynecotokol. 8(4): 32– 35.
- Balk EM, Rofeberg VN, Adam GP, Kimmel HJ, Trikalinos TA, et al. (2019) Pharmacologic and Nonpharmacologic Treatments for Urinary Incontinence in Women: A Systematic Review and Network Meta-analysis of Clinical Outcomes. Annals Internal Medicine. 170(7): 465-479.
- Felde G, Bjelland I, Hunskaar S (2020) Anxiety and depression associated with incontinence in middle-aged women: a large Norwegian cross-sectional study. International Uro- gynecological Journal. 23(3): 299–306.
- Klimaszewska K (2018) The social aspects of urinary incontinence of women. Pielęg.