


Mohammad Hasan Bemanian1, Saba Arshi1, Mohammad Nabavi1, Morteza Fallahpour1, Sima Shokri1, Mina Ahmadi, Fatemeh Atashrazm1, Javad Nazari1, Vahid Bakrani1*
1Department of Allergy and Clinical Immunology, Rasool e Akram Hospital, Iran University of Medical Sciences, Tehran, Iran.
*Corresponding Author: Vahid Bakrani, Department of Allergy and Clinical Immunology, Rasool e Akram Hospital, Iran University of Medical Sciences, Tehran, Iran.
Abstract
Background: It is hard to control chronic urticaria and its complications like itching, which can be the first manifestation of urticaria and cause a disturbance in the patient's quality of life. Opioid antagonist drugs such as naltrexone can inhibit itching. This study aimed to investigate the effect of oral naltrexone on chronic urticaria in reducing the severity of symptoms and clinical improvement and improving the quality of life.
Methods and Materials: This study was a double-masked, randomized clinical trial performed on 62 patients with chronic urticaria. Patients were divided into naltrexone (n = 31) and control (n = 31) groups. The intervention group received naltrexone 50 mg capsules daily, and the control group received a placebo for four weeks. Urticarial Activity Score (UAS7) and Visual Analysis Scale (VAS) were used to assess the severity of symptoms (itching and urticaria), and Dermatology Life Quality Index (DLQI) questionnaire was used to determine the quality of life. The patients were compared at the end of the second and fourth weeks.
Results: Mean age of the patients was 38.32 ± 10.76 years. Thirty-six patients (58.1%) were female, and 26 (41.9%) were male. Examination of baseline characteristics of the patients showed that except for angioedema (P = 0.030) and FH (P = 0.031), other variables were not statistically different in the intervention and control groups (P> 0.05). The results also showed that the intervention group's mean Itch, hives, DLQI score, VAS, and UAS7 scores in the second and fourth weeks were significantly lower (P <0.001).
Conclusion: It seems that naltrexone is an effective and safe alternative treatment option to control itching, reduce pain and increase the quality of life in patients with chronic urticaria.
Keywords: Naltrexone, Chronic Urticaria, Itching, UAS7, VAS, DLQI
Introduction
Urticaria is seen as the sudden development of hives or angioedema. Urticaria is characterized by superficial skin edema, mainly surrounded by bright red erythema and accompanied by severe itching or burning sensation. Hives develop within minutes and are transient, as the skin returns to its normal appearance within one to twenty-four hours. Angioedema manifests as painful swelling or burning without itching with less, deep, subcutaneous, or submucosal edema. Usually, angioedema appears as skin-colored or slightly red swellings, and compared to hives, it develops slowly and may last for several days [1]. Acute urticaria is defined by the repeated appearance of urticarial lesions with or without angioedema over up to six weeks. At the same time, the recurrence of lesions for more than six weeks is considered chronic urticaria [2].
Unexpectedly, the time from the onset of chronic urticaria to proper diagnosis and management is usually long, with considerable variation among different countries, e.g., the mean diagnosis time reported for Canada was 24 months [3]. After the correct diagnosis, many patients repeatedly undergo unnecessary tests to identify the cause, often due to the patient's or the doctor's incorrect understanding of the cause of the disease, such as type I hypersensitivity reactions like food allergies. In addition, consuming many medical resources without results leads to significant frustration in more than 67 % of patients [4]. Chronic urticaria is considered a self-limiting disease, and it has a long duration and may recur over time. Among adults, the mean duration of chronic urticaria is estimated to be 11.5 years, with a recovery of 20-74 % within one year and 30-55 % within five years [5].
The effects of chronic urticaria go beyond physical symptoms and significantly reduce the quality of life of affected people. In one-third of patients, chronic urticaria is associated with depression, anxiety, itching, and sleep disorders, and patients' performance in daily life, school, and work is often significantly impaired [6]. Studies have been conducted on the effectiveness of naltrexone in reducing itching in various systemic and skin diseases, some of which have reported that it is effective, and some have reported it as having low effectiveness [7]. A systematic review and meta-analysis said that only 39 % of patients with chronic spontaneous urticaria (CSU) responded to standard doses of second-generation H1 blocker antihistamines, and only 63% of those who did not respond to normal doses responded to high doses [8]. Although Omalizumab is the primary third-line treatment for chronic urticaria resistant to second-generation H1 blocker antihistamines, some patients do not respond to this treatment or respond late. Accordingly, more safe and effective alternative treatment options are needed, and the therapeutic approach includes two aspects, "removal and prevention of related stimuli" and "medicinal and symptomatic treatment."
Regarding the effectiveness of naltrexone in the treatment of itching in chronic urticaria, few studies have been conducted in the form of case reports [7] or case series [9], which have confirmed its effectiveness, but clinical trials with placebo have not been conducted in this field. The purpose of this study is to investigate the efficacy of oral naltrexone on chronic urticaria in cases where standard treatments are not responsive and consider the financial burden and side effects of third and fourth-line drugs and the low side effects and effectiveness of naltrexone in the treatment of itching with other causes than urticaria; this medicine seems to be an effective and less complicated medicine for the treatment of itching in urticaria, which reduces the severity of symptoms and clinical improvement and improves the quality of life of patients.
Methods and Materials
This study was a double-blind, randomized clinical trial that investigated the efficacy and safety of oral naltrexone in treating 62 patients with chronic urticaria suffering from insufficient response to the maximum dose of H1 and H2 receptor-blocking antihistamines. The diagnosis was based on clinical criteria and rejection of other differential diagnoses. Urticarial Activity Score (UAS7) and Visual Analogue Scale (VAS) were used to evaluate the severity of symptoms (itching and hives), and the Dermatology Life Quality Index (DLQ1) questionnaire was used to assess the quality of life. The outcomes of this study were changes in the itching status as the primary outcome and changes in the severity of urticaria and quality of life. All patients in both groups first received a common one-week standard treatment (Cetirizine 10mg tablets every 6 hours, Famotidine 40mg tablets every 12 hours, and Montelukast 10mg tablets daily). At the end of the first week, as zero phases, evaluation of the VAS and UAS were performed, and with the start of the intervention, standard H1 and H2 inhibitor antihistamine treatment was continued in both groups. The intervention group received Naltrexone 50 mg capsules, and the control group received placebo medicine for 4 weeks. During the second week and the fourth week, the UAS7 questionnaire was completed, and at the end of the second week and the fourth week, the VAS and DLQI questionnaires were completed.
TheUAS7questionnaire has four options: no (score 0), mild (score 1), moderate (score 2), and severe (score 3) itching, and the number of hives questionnaire has four options without (score 0), less than 20 (grade 1), between 20-50 (grade 2) and more than 50 (grade 3) hives. Both questionnaires are calculated daily (UAS 0-6), and the total of 7 days (UAS7 0-42) is collected at the end of the week. In this study, the response to treatment is classified as severe disease (score 28-42), moderate disease (score 16-27), mild disease (score 5-7), and well-controlled urticaria (score 1-6). This questionnaire has been translated into a simple structure and can be used without validation [10]. The patients indicated the severity of their itching on a 10 cm ruler. In this regard, the patients were categorized as less than 3 (mild), 3-7 (moderate), and 8-10 (severe). Regarding DLQ1, developed by Finlay and Khan, it was validated by Zandi et al. in 2020, and its reliability was reported to be higher than 0.7 using Cronbach's alpha method for the entire questionnaire [11].
The DLQI consists of 10 questions related to the patient's past week about the skin symptoms of the disease (itching, discomfort, pain, or burning), the patient's feelings (embarrassment, confusion, nervousness), daily activities (shopping and housework), type of clothes, social activities, recreation, sports, work and education and interpersonal relationships (relationship with spouse, friends, relatives). Considering that the study had two groups and the primary outcome was UAS7 score, and the minimum significant difference in UAS7 based on Hawro et al.'s study was 11 with a standard deviation of 8.5 [12], considering the type I error of 0.5 and the type II error of 0.2, 25 patients were calculated. Due to the possibility of 20% attrition of selected subjects, the sample size was 31 in each group.
Ethical Issue
The tents of the Declaration of Helsinki conducted the research. The Ethics Committee of Iran, University of Medical Sciences, approved this study. The institutional ethical committee at Iran University of Medical Sciences accepted all study protocols (IR.IUMS.FMD.REC.1400.115). Accordingly, written informed consent was taken from all participants before any intervention. The trial protocol was approved in the Iranian registry of clinical trials (#IRCT20210407050878N1).
Data analysis
Data were described using centrality and dispersion indices. The intention-to-treat approach was used for data analysis. Independent t-tests, chi-square tests, and repeated measure ANOVA through SPSS version 24 did data analysis. Less than 0.05 was considered significant.
Results
The present study was conducted on 62 patients with chronic urticaria referred to Hazrat-e Rasoul Hospital. The mean age of examined patients was 38.32±10.76 years. Sixt-three patients (58.1 %) were female, and 26 (41.9 %) were male. The patients were divided into intervention (n=31) and control (n=31) groups. Examining the demographic and essential characteristics of the patients showed that except for angioedema (P=0.030) and FH (P=0.031), other variables in the two intervention and control groups were not statistically different (P > 0.05).
Table 1: Demographic and basic characteristics of the patients in the intervention and control groups
|
Variable |
Group |
P Value |
||
|
Placebo (n=31) |
Intervention (n=31) |
|||
|
Age (Mean±SD), year |
37.61±12.47 |
39.03±8.88 |
0.608 |
|
|
Gender |
Female |
15(48.4) |
21(67.7) |
0.123 |
|
Male |
16(51.6) |
10(32.3) |
||
|
Comorbidity |
No |
22(71) |
25(80.6) |
0.374 |
|
Yes |
9(29) |
6(19.4) |
||
|
Urticarial Dur (Mean±SD) |
23.70±28.80 |
39.26±57. |
0.190 |
|
|
Angioedema |
No |
17(54.8) |
25(80.6) |
0.030 |
|
Yes |
14(45.2) |
6(19.4) |
||
|
FH |
Normal |
20(64.5) |
28(90.3) |
0.031 |
|
Abnormal |
11(35.5) |
3 (9.7) |
||
The frequency of ESR, ANA, HPYL and AntiTpo variables of the patients in the intervention and control groups was investigated using the chi-square test, and the results showed that the frequecnyof these variables in the intervention and control groups were not statistically significant (P>0.05) (Table 2).
Table 2: Frequecny of ESR, ANA, HPYL and AntiTpo variables of patients in two intervention and control groups
|
Variable |
Group |
P Value |
||
|
Placebo (n=31) |
Intervention (n=31) |
|||
|
ESR |
Normal |
26(83.9) |
27(87.1) |
>0.999 |
|
Abnormal |
5(16.1) |
4(12.9) |
||
|
ANA |
Negative |
27(87.1) |
29(93.5) |
0.671 |
|
Positive |
4(12.9) |
2(6.5) |
||
|
HPYL |
Negative |
24(77.4) |
22(71.0) |
0.562 |
|
Positive |
7(22.6) |
9(29.0) |
||
|
AntiTpo |
Negative |
30(96.8) |
25(80.6) |
0.104 |
|
Positive |
1(3.2) |
6(194.) |
||
The mean variables of WBC, HB, EOS and IgE in the two intervention and control groups were tested using independent t-test, and showed that the mean variables of WBC, HB, EOS and IgE in the two intervention and control groups ere not statistically significant (P > 0.05).
Table 3: Comparison of the mean WBC, HB, EOS and IgE variables in the two intervention and control groups.
|
Variable |
Group |
N |
Mean |
SD |
P value |
|
WBC |
Intervention |
31 |
10705.50 |
16127.26 |
0.538 |
|
Placebo |
31 |
13145.16 |
14598.23 |
||
|
HB |
Intervention |
31 |
13.047 |
2.19 |
0.538 |
|
Placebo |
31 |
12.719 |
1.92 |
||
|
EOS |
Intervention |
31 |
162.800 |
117.24 |
0.366 |
|
Placebo |
31 |
139.839 |
75.77 |
||
|
IgE |
Intervention |
31 |
245.767 |
393.46 |
0.530 |
|
Placebo |
31 |
197.484 |
140.19 |
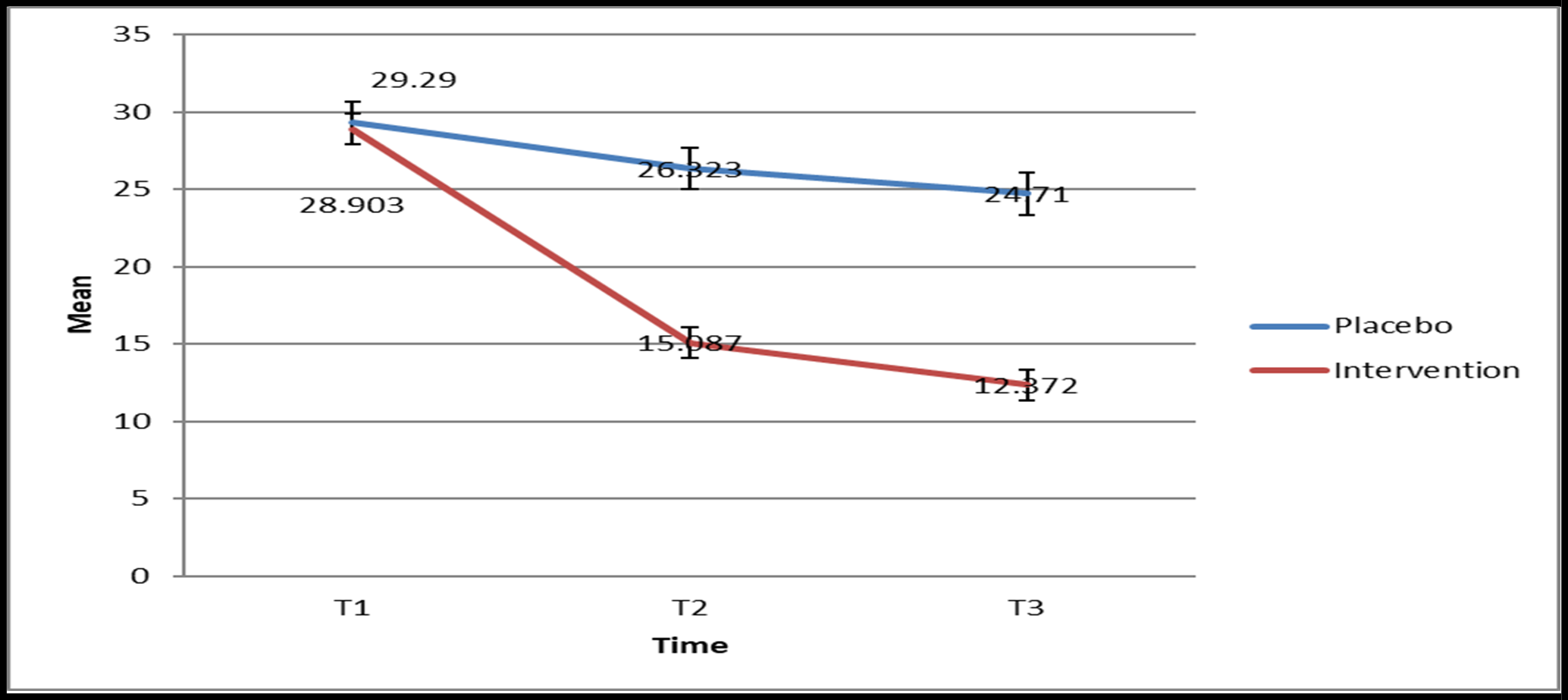
The mean score of Itch at three times T1, T2 and T3 in the intervention and control groups was checked using repeated measures ANOVA test. The results showed that the mean score of Itch at three times T1, T2 and T3 in two intervention and control groups had significant changes (P>0.001). Also, the results of intergroup effects in both intervention and control groups showed that the changes between the two groups were statistically significant (P>0.001). The comparison results in the mentioned times showed that the mean Itch score in times T2 and T3 was significantly lower in the intervention group (P<0.001) (Figure 1).
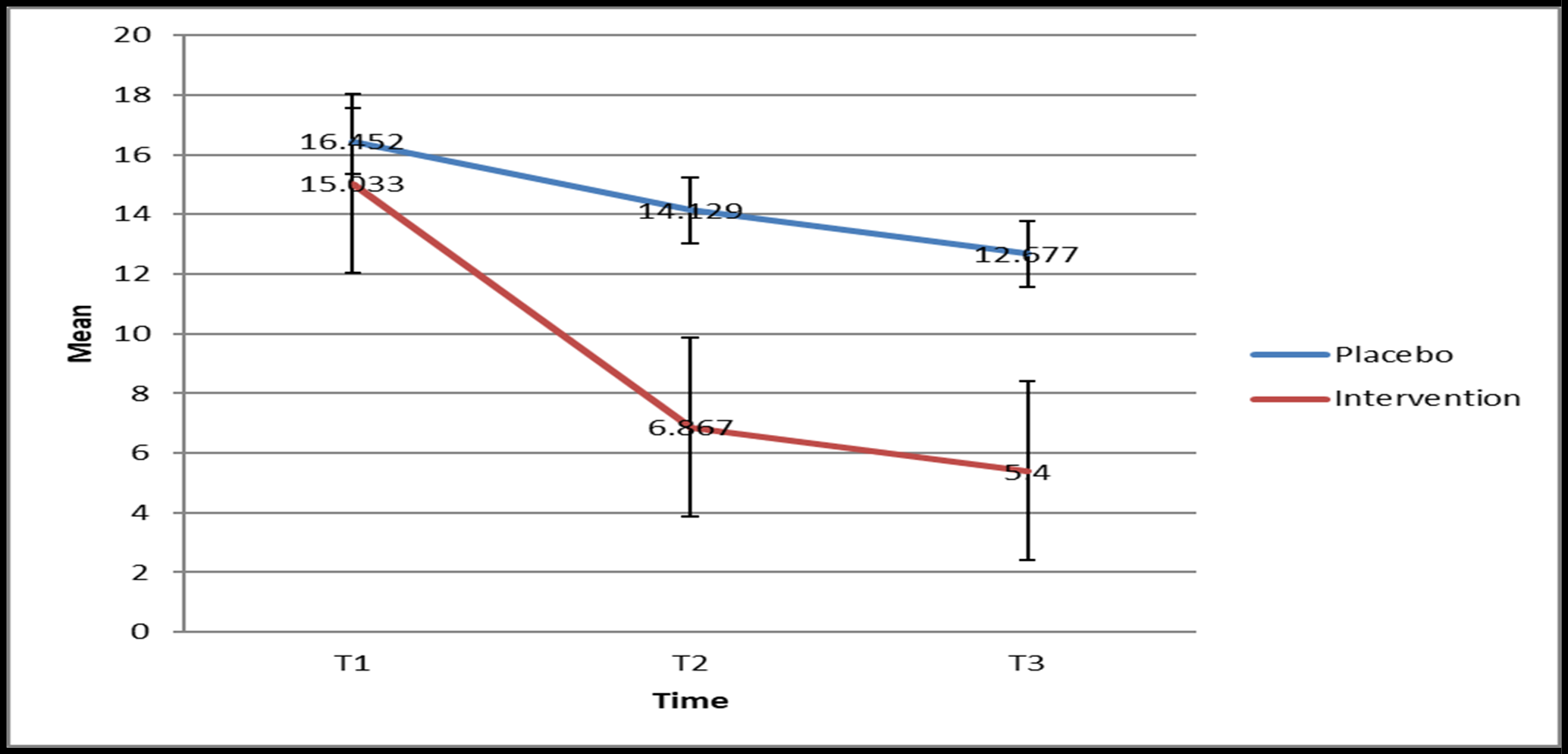
Figure 1: Trend of Itch score of the patients at three times T1, T2 and T3 in the intervention and control groups
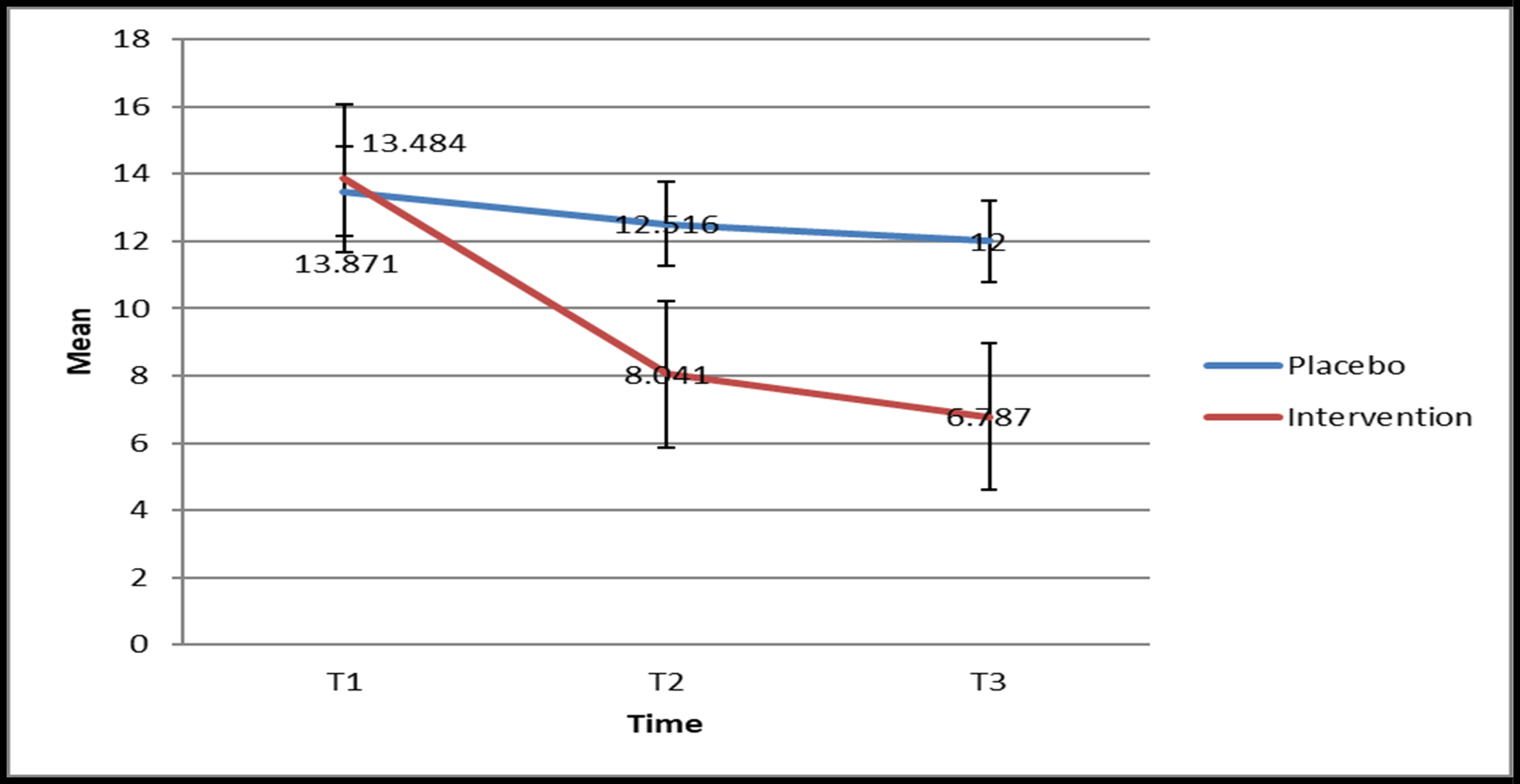
Figure 2: Trend ofhives score of the patients at three times T1, T2 and T3 in the intervention and control groups.
The mean score of DLQIat three times T1, T2 and T3 in the intervention and control groups was checked using repeated measures ANOVA test. The results showed that the mean score of DLQIat three times T1, T2 and T3 in two intervention and control groups had significant changes (P>0.001). Also, the results of intergroup effects in both intervention and control groups showed that the changes between the two groups were statistically significant (P>0.001). The comparison results in the mentioned times showed that the meanDLQIscore in times T1, T2 and T3 was significantly lower in the intervention group (P<0.001) (Figure 3).
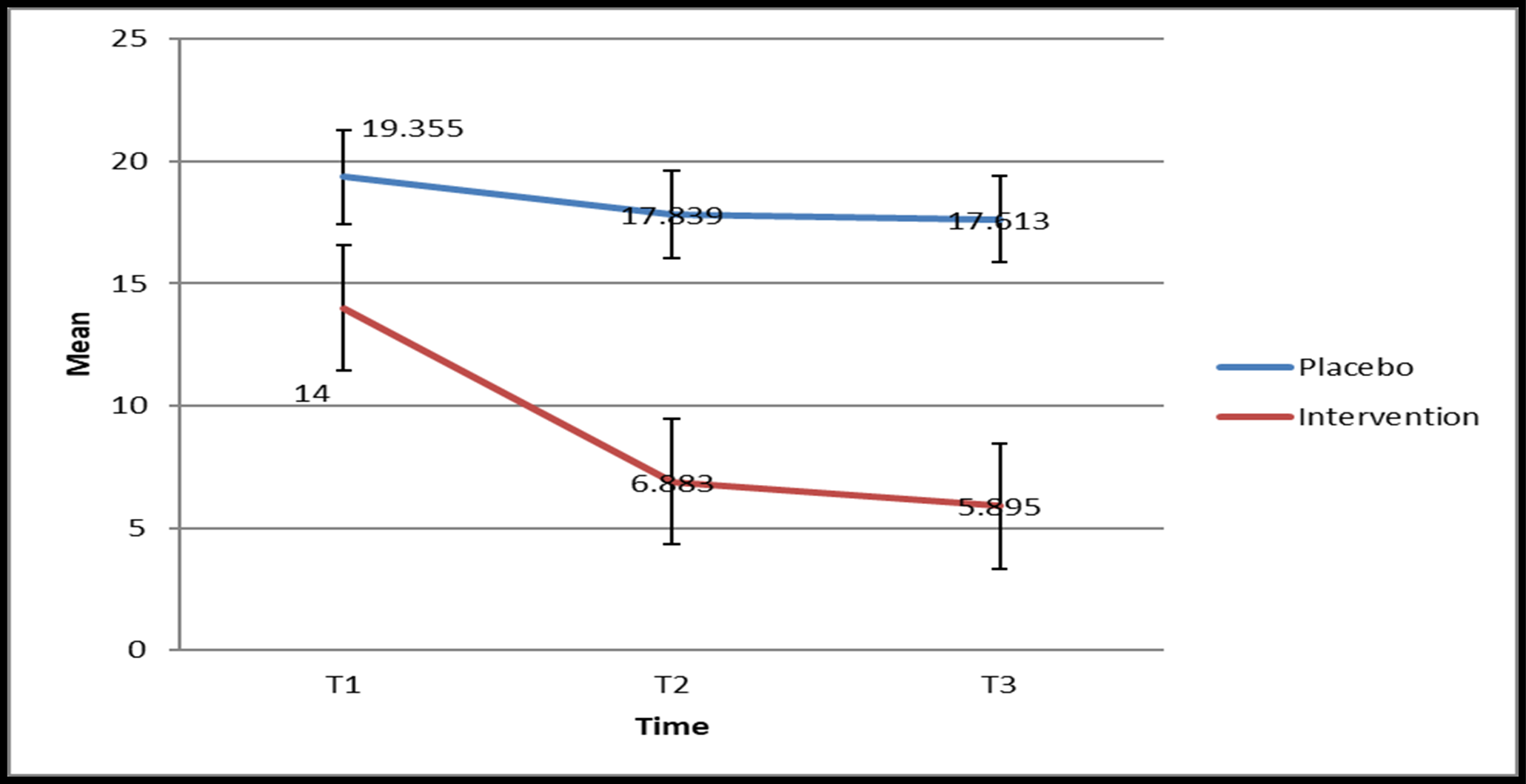
Figure 3: Trend ofDLQI score of the patients at three times T1, T2 and T3 in the intervention and control groups.
The mean score of VASat three times T1, T2 and T3 in the intervention and control groups was checked using repeated measures ANOVA test. The results showed that the mean score of VASat three times T1, T2 and T3 in two intervention and control groups had significant changes (P>0.001). Also, the results of intergroup effects in both intervention and control groups showed that the changes between the two groups were statistically significant (P>0.001). The comparison results in the mentioned times showed that the meanVASscore in times T2 and T3 was significantly lower in the intervention group (P<0.001) (Figure 4).
The mean score of VASat three times T1, T2 and T3 in the intervention and control groups was checked using repeated measures ANOVA test. The results showed that the mean score of VASat three times T1, T2 and T3 in two intervention and control groups had significant changes (P>0.001). Also, the results of intergroup effects in both intervention and control groups showed that the changes between the two groups were statistically significant (P>0.001). The comparison results in the mentioned times showed that the meanVASscore in times T2 and T3 was significantly lower in the intervention group (P<0.001) (Figure 4).
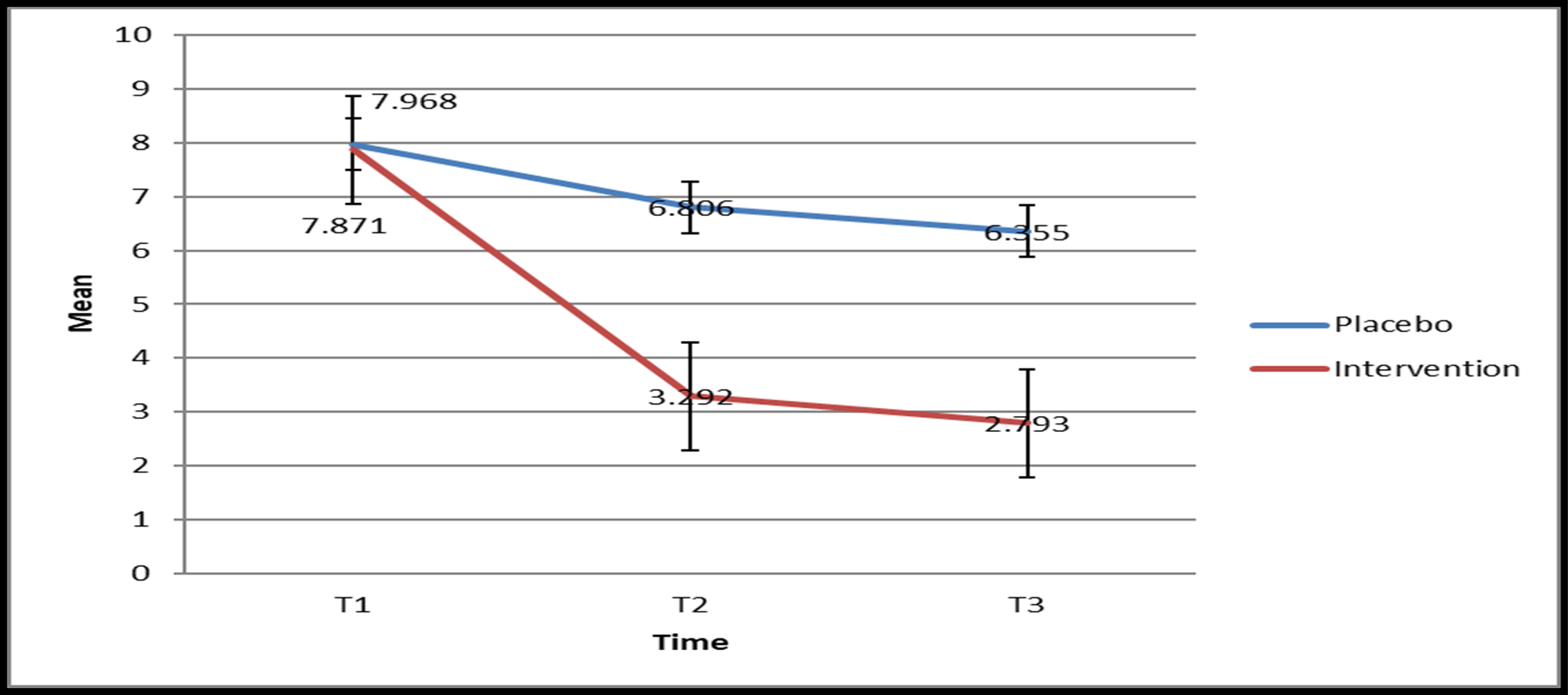
Figure 4: Trend of VAS score of the patients at three times T1, T2 and T3 in the intervention and control groups.
The mean score of UAS7at three times T1, T2 and T3 in the intervention and control groups was checked using repeated measures ANOVA test. The results showed that the mean score of UAS7at three times T1, T2 and T3 in two intervention and control groups had significant changes (P>0.001). Also, the results of intergroup effectsin both intervention and control groups showed that the changes between the two groups were statistically significant (P>0.001). The comparison results in the mentioned times showed that the meanUAS7 score in times T2 and T3 was significantly lower in the intervention group (P<0.001) (Figure 5).
Discussion
Studies conducted to investigate the effectiveness of naltrexone in the treatment of itching in chronic urticaria have been carried out in the form of case reports [7] or case series [9], and these studies have confirmed its effectiveness, but clinical trials with placebo not done in this field. In a case report presented by Asli Aytulum et al., a 78- year-old woman with chronic and treatment-resistant itching who was referred from a dermatology clinic with the diagnosis of chronic psychogenic urticaria was investigated. According to the lack of the presence of an underlying cause in the tests and the absence of response to routine anti-itching drugs such as antihistamines and insufficient response to serotonergic medications such as citalopram, they were treated with 25 mg of naltrexone daily, and shortly after the start of the drug, the patient's symptoms ultimately improved [7]. The results of the present study also showed that receiving naltrexone significantly reduces itching in patients. Some clinical studies and case reports suggest that naltrexone may be effective in pruritus [13,14]. Possible mechanisms in opioid-treated itching include direct binding to opioid receptors in the central nerve system and interactions with serotonin or 5-hydroxytryptamine receptors. Reduction of itching with opioid antagonists also suggests that histamine release is not the only mechanism of opioid-induced itching but that μ-opioid receptors are also involved in the centrally mediated response [15]. In a case series report presented by Lipener et al. in 2020, 16 patients with severe itching resistant to treatment with different etiologies, including chronic urticaria, were treated with Bupropanol, agonist-antagonist of opioid receptors, in the form of inhalation spray (10 mg/ml). Thirteen out of 16 patients (81 %) showed a significant improvement in itching six weeks after the start of treatment, one patient had no change, and 2 patients refused to continue treatment without an apparent reason [9]. In a study by Lee et al. in 2016 to investigate the effect of oral naltrexone on itching in elderly patients with chronic pruritus resistant to conventional treatments, 18 patients with a mean age of 70 years with antihistamine-resistant itching and underlying causes different (itching caused by cholestasis, uremia, old age eczema, psoriasis, lymphoma and itching of unknown cause) were treated with naltrexone 50 mg daily for two months. Baseline tests were sent to all patients, and the effect of medication on itching was evaluated based on VAS. 13 of these people (equivalent to 72.2 %) showed a significant improvement in itching in the form of a reduction of more than 50 % in the amount of itching based on VAS, of which 6 people (equivalent to 33 %) showed a complete improvement in symptoms with VAS score of zero and ones well as two patients (11 %) did not improve significantly [16].
The results of the present study showed that the mean VAS score was significantly lower in the intervention group. It has been previously reported that endogenous or exogenous opioids can induce or exacerbate itching [17–19]. There is general agreement that opioids often produce an analgesic effect in combination with itching stimulation. However, a recent study showed that morphine-induced long-term itch occurs independently via the μ-opioid receptor and morphine-induced analgesia [19]. In a review article by Quan Phan et al., 550 patients with different causes of itching were studied. A significant effect of Mu opioid receptor antagonists was reported to improve itching symptoms in these patients with naloxone and naltrexone [20]. The findings of this study were consistent with the present study. In the clinical trial study by Dieter Metez et al., the effect of oral naltrexone on the treatment of itching with different causes (dermatological and internal causes) was performed on 50 patients. In this study, 50 patients were treated with oral naltrexone 50 mg daily for four weeks. The effect of naltrexone on itching was evaluated based on VAS evaluation. Thirteen patients out of 50 studied (26 %) recovered from itching. Thirteen patients (26 %) showed more than 50 % improvement, nine people (18 %) showed less than 50 % improvement, and 15 patients (30 %) showed no change in symptoms [21].
Lee et al. assessed the efficacy and safety of naltrexone on 18 patients and showed that naltrexone improves the VAS score of patients; also, more than 50 % of patients reported a decrease in itching intensity, and the symptoms of most patients (88.9 %) improved. Only patients (11.1 %) had persistent itching. Five patients reported side effects, including insomnia, fatigue, constipation, and anorexia [14]. However, reactions were either limited to the first two weeks or were well managed. As Lee et al. reported, naltrexone reduced pain and itching and was consistent with the results of the present study. Naltrexone is a synthetic compound of oxymorphone that blocks the effects of opioids twice as much as naloxone. Naltrexone displaces endorphins at μ- and κ-receptors and shows minimal pharmacological activity.
Furthermore, naltrexone has a high oral bioavailability and shows a linear increase in the area under the plasma concentration-time curve. It is only contraindicated in patients with acute hepatitis, liver failure, and severe liver failure and should not be used in children, pregnant or lactating women [22]. Naltrexone has no abuse potential because it does not cause physical dependence [14].
Conclusion
It seems that naltrexone is an effective and safe alternative treatment option to control itching, reduce pain and increase the quality of life in patients with chronic urticaria.
References
- Zuberbier T, Aberer W, Asero R, Bindslev-Jensen C, Brzoza Z, et al (2014) The EAACI/GA2LEN/EDF/WAO Guideline for the definition, classification, diagnosis, and management of urticaria: the 2013 revision and update. Allergy. 69(7): 868–887.
- Magerl M, Altrichter S, Borzova E, Giménez-Arnau A, Grattan CE, et al. (2016) The definition, diagnostic testing, and management of chronic inducible urticarias—the EAACI/GA(2) LEN/EDF/UNEV consensus recommendations 2016 update and revision. Allergy. 71(6): 780–802.
- Maurer M, Abuzakouk M, Bérard F, Canonica W, Oude Elberink H, et al. (2017) The burden of chronic spontaneous urticaria is substantial: Real-world evidence from ASSURE-CSU. Allergy. 72(12): 2005–16.
- Williams PV, Kavati A, Pilon D, Xiao Y, Zhdanava M, et al. (2018) Treatment Patterns, Healthcare Resource Utilization, and Spending Among Medicaid-Enrolled Children with Chronic Idiopathic/Spontaneous Urticaria in the United States. Dermatol Ther. 8(1): 69–83.
- Eun SJ, Lee JY, Kim DY, Yoon HS (2019) Natural course of new-onset urticaria: Results of a 10-year follow-up, nationwide, population-based study. Allergol Int. 68(1): 52–8.
- Mann C, Dreher M, Weeß HG, Staubach P (2020) Sleep disturbance in patients with urticaria and atopic dermatitis: an underestimated burden. ActaDermVenereol. 100(6): adv00073.
- Aytulun A, Ozcelik-Eroglu E, Yildiz MI, Armagan BY, Yazici MK (2020) Oral Naltrexone in the Treatment of Chronic Psychogenic Pruritus: A Case Report. Psychiatry and Clinical Psychopharmacology. 30(2): 199-201.
- Guillen-Aguinaga S, Jauregui Presa I, Aguinaga-Ontoso E, Guillen-Grima F, Ferrer M (2016) Updosing nonsedating antihistamines in patients with chronic spontaneous urticaria: a systematic review and meta-analysis. Br J Dermatol. 175(6): 1153-1165.
- Khanna R, Kwon CD, Patel SP, Belzberg M, Williams KA, et al. (2020) Intranasal butorphanol rescue therapy for the treatment of intractable pruritus: A case series. J Am Acad Dermatol. 83(5): 1529-1533.
- Zandi S, Shamsi Meymandi S, Hasheminasab Gorji S, Sabouri Shahrebabak F (2011) Evaluation of quality of life in patients with psoriasis. J Dematol Cos. 2(3): 166-173.
- Balp MM, Lopes da Silva N, Vietri J, Tian H, Ensina LF et al. (2017) The Burden of Chronic Urticaria from Brazilian Patients ’ Perspective. Dermatol Ther. 7(4): 535–45.
- Hawro T, Ohanyan T, Schoepke N, Metz M, Peveling-Oberhag A, et al. (2018) The Urticaria Activity Score-Validity, Reliability, and Responsiveness.J Allergy Clin Immunol Pract. 6(4): 1185- 1190.e1.
- Metze D, Reimann S, Beissert S, Luger T (1999) Efficacy and safety of naltrexone, an oral opiate receptor antagonist, in the treatment of pruritus in internal and dermatological diseases. Journal of the American Academy of Dermatology. 41(4): 533-9.
- Lee J, Shin JU, Noh S, Park CO, Lee KH (2016) Clinical efficacy and safety of naltrexone combination therapy in older patients with severe pruritus. Annals of Dermatology. 28(2): 159-63.
- Kumar K, Singh SI (2013) Neuraxial opioid-induced pruritus: an update. Journal of anaesthesiology, clinical pharmacology. 29(3): 303-307.
- Lee J, Shin JU, Noh S, Park CO, Lee KH (2016) Clinical Efficacy and Safety of Naltrexone Combination Therapy in Older Patients with Severe Pruritus. Ann Dermatol. 28(2): 159-63.
- Liu XY, Liu ZC, Sun YG, Ross M, Kim S, et al. (2011) Unidirectional cross-activation of GRPR by MOR1D uncouples itch and analgesia induced by opioids. Cell. 147(2): 447-58.
- Ständer S, Steinhoff M, Schmelz M, Weisshaar E, Metze D, et al. (2003) Neurophysiology of pruritus: cutaneous elicitation of itch. Archives of dermatology. 139(11): 1463-70.
- Blunk JA, Schmelz M, Zeck S, Skov P, Likar R, et al. (2004) Opioid-induced mast cell activation and vascular responses is not mediated by μ-opioid receptors: an in vivo microdialysis study in human skin. Anesthesia & Analgesia. 98(2): 364-70.
- Phan NQ, Bernhard JD, Luger TA, Ständer S (2009) Antipruritic treatment with systemic μ-opioid receptor antagonists: a review. J Am Acad Dermatol. 8: 52.
- Metze D, Reimann S, Beissert S, Luger T (1999) Efficacy and safety of naltrexone, an oral opiate receptor antagonist, in the treatment of pruritus in internal and dermatological diseases. J Am Acad Dermatol. 41(4): 533-9.
- Phan NQ, Bernhard JD, Luger TA, Ständer S (2010) Antipruritic treatment with systemic μ-opioid receptor antagonists: a review. J Am Acad Dermatol. 63: 680-8.