


Zohaib Ahmed1, Naima Amir Zaman2*, Muhamad Rafay3, Rabia Ali4
1Liaquat National Hospital, Pakistan
2Agha Khan University, Pakistan
3Liaquat National Hospital
4Liaquat National Hospital
*Corresponding Author: Naima Amir Zaman, Agha Khan University, Pakistan
Abstract
Background
Olfactory neuroblastoma (esthesioneuroblastoma) is a rare malignant tumor originating from the olfactory neuroepithelium of the nasal cavity. It accounts for about 2% of all sino-nasal neoplasms, with an estimated incidence of 0.4 cases per million population. The tumor most commonly presents in the fifth decade of life, typically with nasal obstruction, epistaxis, or, less often, anosmia and facial pain. Due to its nonspecific presentation, diagnosis is often delayed, requiring a high index of suspicion and multidisciplinary management.
Case Presentation
A 50-year-old female with no known comorbidities presented with a one-year history of progressive nasal obstruction and intermittent epistaxis. There were no visual disturbances, headaches, or facial swelling. Examination revealed a mass occupying the nasal cavity. Radiological imaging demonstrated a soft tissue lesion arising from the superior nasal cavity and extending toward the cribriform plate. Histopathological analysis confirmed the diagnosis of olfactory neuroblastoma.
Management And Outcomes
The patient underwent surgical resection of the tumor followed by adjuvant chemotherapy. Her postoperative course was uneventful, and follow- up imaging showed no residual or recurrent disease. She continues regular follow-up with satisfactory recovery until after approximately 1.5 months, she developed persistent headaches. Further workup revealed metastatic disease necessitating the need of surgical intervention and a more aggressive treatment plan.
This case highlights the importance of timely diagnosis and combined surgical and chemotherapeutic management involved in olfactory neuroblastoma treatment.
Conclusion
Early diagnosis and comprehensive management, along with the timely involvement of a multidisciplinary team, are essential for achieving favorable outcomes in olfactory neuroblastoma neuroblastoma and more clinical trials should be done to treat the refractory diseases.
Key Clinical Message
Even vague symptoms such as nasal obstruction and intermittent epistaxis may signal an underlying olfactory neuroblastoma. Early recognition and timely multidisciplinary management with surgery and adjuvant therapy can achieve favorable outcomes, even in cases with intracranial extension.
Introduction
Olfactory neuroblastoma is a rare malignant tumor of nasal cavity . It starts from a nerve called olfactory nerve which primarily regulates your sense of smell [1]. These tumors involve the bone of the skull situated between the eyes ( cribriform plate ) . The cause of this tumor is unknown and there is no identifiable risk factor for these kind of tumors . These tumors occur over a wide range ( 3 to 90 years ),with a bimodal peak between the second and third decade and a second peak in the sixth and seventh decades [2]. The presenting complaints of olfactory neuroblastoma may vary and can include nasal obstruction, headache, anosmia, epistaxis, or, in rare cases, ocular manifestations. These may present as severe bilateral papilledema, engorged and tortuous retinal veins, and decreased visual acuity [2]. The differential diagnosis of olfactory neuroblastoma must include Sino-nasal undifferentiated carcinoma, nasal melanoma, nasal squamous cell carcinoma and meningioma [3]. The behavior of ONB can vary widely, ranging from a less aggressive tumor associated with long-term survival to a highly aggressive form characterized by distant metastasis and reduced life expectancy [4]. MRI and endoscopic biopsy are standard diagnostic modalities of choice in the case of olfactory neuroblastoma. According to most studies, the preferred treatment approach involves surgical resection followed by chemo-radiotherapy. In a retrospective review of approximately 129 patients, 82 underwent surgical resection alone, while the remaining patients received surgical resection followed by either chemotherapy or concurrent chemo-radiotherapy. The five-year overall survival and disease-specific survival rates reported were 85.6% and 93.4%, respectively [4]. The objective of this case report is to highlight the diagnostic challenges, management strategies, and the need for clearer guidelines to prevent recurrence of olfactory neuroblastoma, supported by current literature and similar case presentations.
Classification
The modified Kadish system (which added category D to the original Kadish System) is shown below [5]
|
Modified Kadish |
Biller et al |
Dulguerov and Calcattera |
|
A: Confined to nasal cavity |
T1: Nasal/ paranasal sinuses |
T1: nasal/paranasal sinuses |
|
B: Extends to paranasal sinus |
T2: Periorbital/anterior fossa extension |
T2: Erosion of cribriform plate |
|
C: local extension (orbit or cribriform plate) |
T3: Brain involvement, resect able margins |
T3: Periorbital/anterior fossa extension |
|
D: Distant metastasis |
T4: Unable to obtain negative margins (unresectable) |
T4: Brain involvement |
This classification systems appears to correlate with survival. Alternative systems by Biller et al and Dulguerov and Calcaterra attempt to subdivide the Kadish C classification; however, the more popular modified Kadish system is more frequently used [1]
Case Report
A 50-year-old female presented to the ENT outpatient department with a one-year history of progressive left-sided nasal obstruction and intermittent epistaxis, which responded partially to medical treatment. The symptoms were also associated with anosmia and rhinorrhea. On systemic examination, bilateral nasal patency was reduced, more pronounced on the left side. Anterior rhinoscopy revealed a fleshy mass occupying the left nasal cavity with blood- tinged discharge, which did not bleed on touch. There was a deviation of the nasal septum to the right. Visual acuity was decreased as she had bilateral cataracts which is unlikely to be seen in a patient with ONB, and funduscopic findings were unremarkable. However, physical examination revealed bilateral exophthalmos, while the remainder of the systemic examination was within normal limits. The patient was admitted for further diagnostic workup, including MRI of the brain with contrast. The neurosurgery team was consulted and histopathological evaluation was planned to confirm the diagnosis.
Radiological And Histopathological Features
A computed tomography (CT) scan of the paranasal sinuses (PNS), both plain and contrast-enhanced, was performed to evaluate persistent epistaxis and rule out other underlying pathologies. The imaging revealed complete opacification of the left frontal, ethmoid, maxillary, and sphenoid sinuses, with mild post-contrast enhancement. There was mild extension of the lesion into the right ethmoid sinus and the left nasal cavity. Additional findings included remodeling of the ethmoidal septa, widening of the osteo-meatal complex, and deviation of the nasal septum towards the right side. The initial radiological impression was suggestive of a Sino nasal polyp.
A biopsy of the lesion was subsequently performed. Histopathological examination revealed a malignant neoplasm. Immuno-histochemical staining demonstrated positivity for cytokeratin, synaptophysin, and CD56, with focal positivity for P63. Synaptophysin which is a reliable marker of neoplastic neuroendocrine cell and is normally found in synaptic vesicles of neurons and contains important role in diagnosing ganglio-neuromas, neuroblastomas, para-gangliomas, and small cell carcinomas, while Cytokeratin indicates the epithelial nature of the lesion. The tumor cells were negative for P40. The immune-profile was consistent with a diagnosis of olfactory neuroblastoma.
Further imaging with magnetic resonance imaging (MRI) of the brain with and without contrast was performed for surgical planning and staging. The MRI revealed a large, heterogeneously enhancing mass centered in the region of the left ethmoid sinuses, with intracranial extension into the left frontal lobe through a widened cribriform plate as shown in (Figure 1 and 2). Additionally, an enlarged enhancing left cervical level IB lymph node was identified, suggestive of possible regional metastasis. No leptomeningeal or intra- parenchymal post-contrast enhancement was noted.
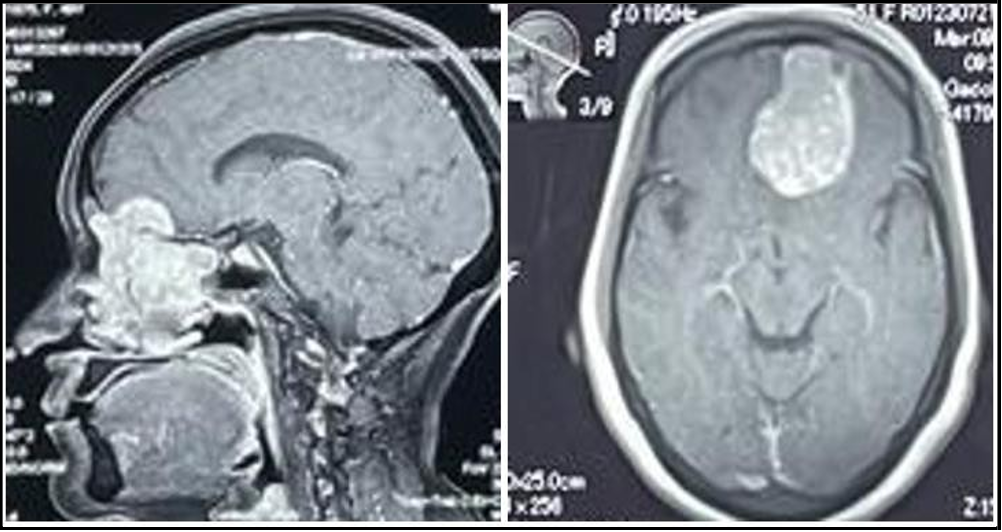
Figure 1 and 2: Coronal and Axial sections of MRI Brain with contrast showing intracranial extension of olfactory neuroblastoma into left frontal lobe
Following the confirmation of olfactory neuroblastoma and the findings of intracranial extension and possible nodal metastasis on MRI, a multidisciplinary team (MDT) meeting was conducted. The MDT included specialists from otolaryngology-head and neck surgery, neurosurgery and oncology. After thorough review of the clinical, radiological, and histopathological findings, a consensus was reached to proceed with surgical resection of the tumor as the initial treatment modality, followed by further oncological evaluation for adjuvant therapy planning. The involvement of both ENT and neurosurgical teams was deemed essential due to the tumor’s transcranial extension through the cribriform plate into the anterior cranial fossa. Given the suspicion of cervical nodal metastasis, a whole-body positron emission tomography-computed tomography (PET-CT) scan was advised to assess for distant metastatic spread and guide further management. The PET-CT scan revealed no evidence of hypermetabolic metastatic lesions in the liver, adrenal glands, lungs, or bony skeleton, thereby excluding distant metastasis at the time of staging.
Following a consensus by the multidisciplinary team, surgical intervention was chosen as the primary mode of treatment. On 15 March 2024, she underwent Endoscopic intranasal excision of tumor along with Bifrontal craniotomy and excision. The procedure was uneventful, with no intraoperative complications. Complete resection of the tumor was achieved with no visible residual tissue. A sample was sent for histopathological examination. Post-operatively, the patient remained hemodynamically and vitally stable and was discharged home in good condition with follow-up in the neurosurgery and oncology clinic with the final biopsy report. The final biopsy report confirmed the diagnosis of olfactory neuroblastoma Grade 4. Based on these findings, the oncology team was consulted and they emphasized the potential need for adjuvant radiotherapy depending on tumor type, grade, and molecular markers. The patient was continuing to be monitored closely through regular follow-up appointments with neurosurgery and oncology teams. As per the recommendation of her oncologist, the patient was scheduled to undergo a 35-40 radiation therapy cycles of Gamma radiation. She ultimately completed 35 radiation cycles over the course of 10 months.
Reoccurrence
She began experiencing relapsing symptoms, including persistent headaches lasting for a week, prompting a neurosurgical evaluation to assess the possibility of recurrence of his previously diagnosed condition. A contrast-enhanced MRI of the brain was performed to evaluate for any mass effect that could account for the headaches. On physical examination, papilledema was noted, and signs of raised intracranial pressure (ICP) were confirmed on MRI. MRI Brain plain and contrast reveals two heterogeneously enhancing lesions in the right anterior fronto-parietal regions (Figure 3 and 4). Both lesions were found to be overlapping each other. First lesion is larger solid cum cystic, extra axial showing avid heterogeneous post contrast enhancing lesion along right anterior parietal convexity causing effacement of right lateral ventricle and vasogenic edema surrounding brain parenchyma. Second smaller lesion showing bony infiltration of the overlying anterior parietal skull vault, extraaxial and slightly hypo enhancing.
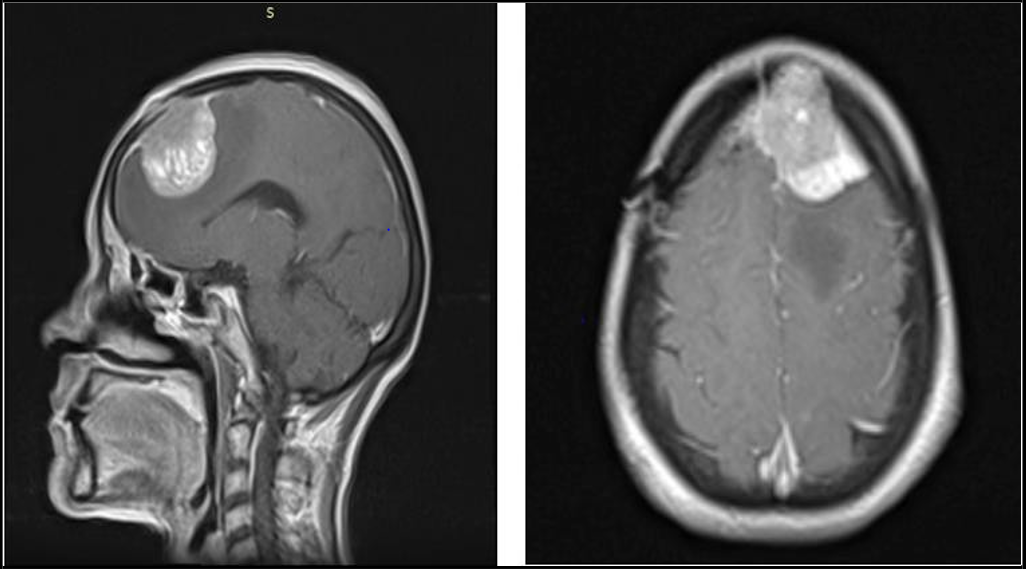
Figure 3 and 4: MRI Brain with contrast showing coronal and Axial views revealing an extra axial neoplastic metastatic lesion seen along the right anterior parietal convexity with contralateral midline shift of 9.8mm.
Approximately 15 months later, on 6 June 2025, a second surgery was planned to resect the newly recurrent metastatic lesion. The patient subsequently underwent a frontal craniotomy with excision of the space-occupying lesion, aiming to achieve safe maximal resection. The procedure was completed successfully without any intraoperative complications. Postoperatively, the patient's symptoms of raised intracranial pressure resolved. She was initiated on corticosteroids to reduce cerebral edema, which were gradually tapered off. She was advised to follow up closely with her oncologist for long-term surveillance and to assess the need for more extensive radiation therapy during this recurrence. A biopsy of the excised lesion was performed, the details of which are provided in the figure below (Figure 5).
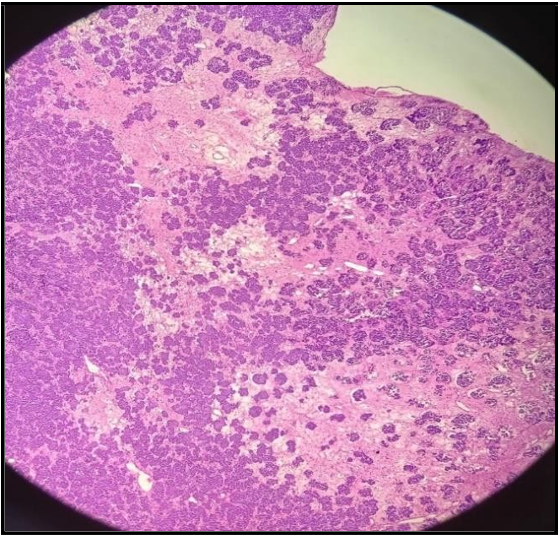
Figure 5: Showing morphological features of olfactory neuroblastoma exhibiting lobulated growth with nests and clusters of small round blue cells.
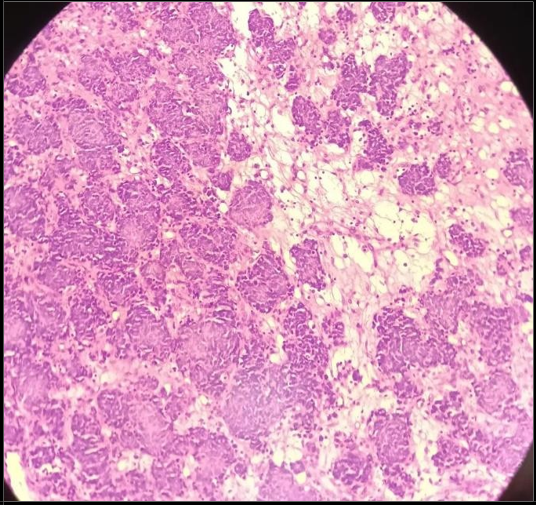
Figure 6: The tumor cells show hyperchromatic rounded nuclei with scanty cytoplasm.
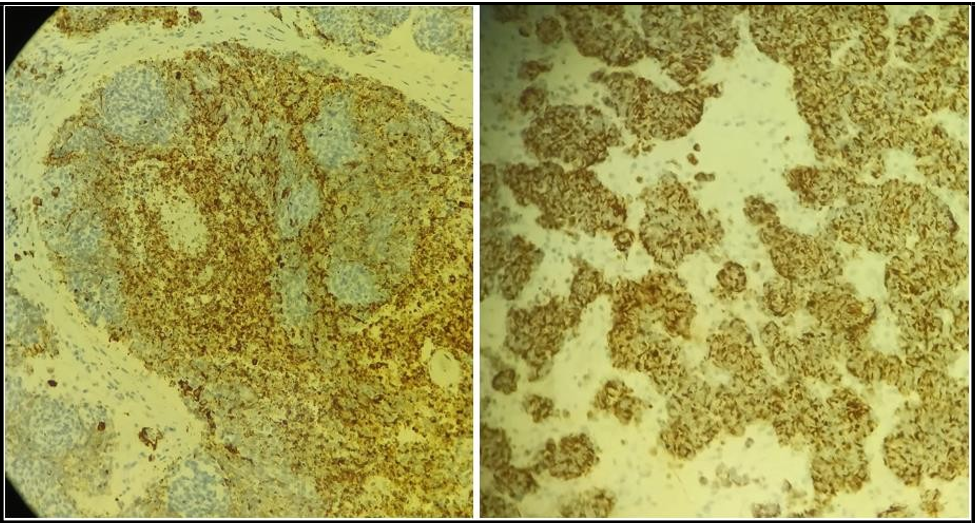
Figure 7 and 8: Showing Immunohistochemistry of olfactory neuroblastoma .The tumor cells are positive for CD-56,synaptophysion(indicating neuroendocrine origin), calretinin and diffuse positivity for CKAE1/AE3 which indicates endothelial components of carcinoma.
Discussion
Olfactory neuroblastoma and its diagnosis is often challenging due to its overlapping clinical and histological features with other neuroendocrine tumors. This diagnostic difficulty frequently leads to delayed medical management and, in many cases, metastatic spread by the time of diagnosis. Such delays highlight the importance of heightened clinical suspicion and early diagnostic intervention in this rare but potentially lethal tumors. Despite timely diagnosis and prompt treatment, olfactory neuroblastoma is known for its tendency to recur. The current gold standard for management typically involves surgical resection followed by adjuvant radiotherapy. However, the risk of recurrence remains particularly high in patients with poor prognostic indicators, such as high Hyams grade, advanced Kadish stage, and positive surgical margins [6].
Studies have shown that most recurrences occur between 5 to 10 years after the initial presentation. As reported in other case studies, it is common for metastatic lesions to be detected approximately two years after the initial diagnosis of olfactory neuroblastoma [7].
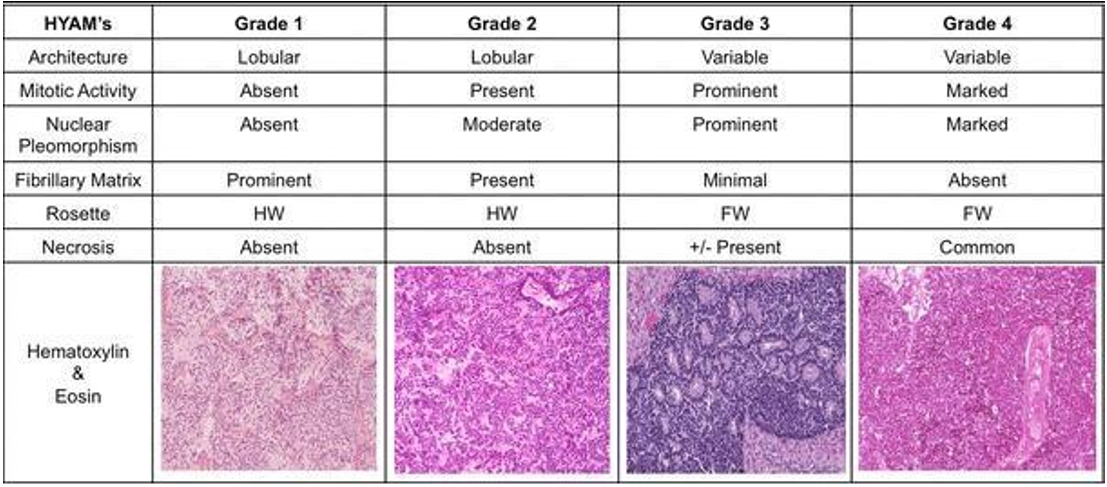
Although olfactory neuroblastoma is considered radiosensitive and responds well to radiation therapy, recurrence rates are not significantly reduced by radiation alone [7]. Therefore, long-term follow-up and multimodal treatment strategies are crucial in improving outcomes in these patients. The chart below explained the HYAMs grading in the easiest manner:
Olfactory neuroblastoma tends to metastasize rapidly, particularly due to its potential for early extension into intracranial structures via the cribriform plate. Involvement of the cribriform plate and orbit is recognized as an important prognostic factor. Studies have reported a cervical lymph node involvement rate of approximately 20%, a local recurrence rate of 20–30%, and a distant metastasis rate of up to 50% within the first six months following diagnosis [8]. These aggressive patterns of spread underscore the importance of early detection and comprehensive treatment planning [8].
In a study involving 28 patients conducted by Aboziada and Eisbruch [9] the addition of radiotherapy following successful craniofacial resection was shown to significantly reduce the risk of recurrence. Among the patients who received postoperative radiotherapy, only 2 out of 13 experienced recurrences, whereas recurrences occurred in 11 out of 16 patients who did not receive additional radiotherapy [8, 9].
However, it is important to note that these findings are based on a relatively small sample size, and there remains limited high-quality evidence to definitively establish the benefit of postoperative radiotherapy. Larger, controlled studies are needed to validate these results and guide treatment protocols. Another study by Benfari et al. emphasizes the importance of combining radiotherapy with chemotherapy as a routine approach for treating stage C olfactory neuroblastoma [8]. The study suggests that radiotherapy alone should be reserved for cases where the tumor is confined to the cribriform plate without evidence of bony destruction. However, the overall management of olfactory neuroblastoma remains challenging due to the lack of clear, standardized treatment protocols. This uncertainty, coupled with a scarcity of statistically robust data, contributes to the disease’s poor prognosis and unfavorable outcomes in many patients [10].
Considering the role of chemotherapy few studies have been reported to evaluate the efficacy of chemotherapy in patients with recurrent or advanced esthesioneuroblastoma (Kadish Stage C). A retrospective study including 10 patients highlights the role of adjuvant chemotherapy for both high grade and low-grade tumors which reveals that platinum based chemotherapy causes notable tumor regression in the high grade tumors with the mean duration of 9.3 months highlighting the short-term yet meaningful benefit in improving the survival time [11]. Despite of lacking a clearer guidelines regarding the prompt treatment and role of adjuvant chemo radiation therapy in preventing the recurrence. Diagnosis and management of olfactory neuroblastoma has improved significantly in the last three decades. [3]
A retrospective case series reported on 11 patients, of whom 6 received immune checkpoint inhibitors such as PD-L1 inhibitors, while 5 did not. The use of PD-L1 inhibitors was associated with an approximate increase in survival of 6.4 months. However, the adverse effects of these medications remain inadequately understood, and their use is not yet widespread globally. This highlights the need for well-designed randomized controlled trials (RCTs) to establish their safety and efficacy. [12]
In this case, despite prompt treatment, complete surgical resection with negative margins, and completion of 35 cycles of radiotherapy, the tumor recurred aggressively.
Conclusion
Further studies and clinical trials are needed to establish standardized treatment guidelines and develop strategies to prevent recurrence. In this particular case, the patient underwent complete tumor resection followed by 35 cycles of radiation therapy, along with prompt follow- up. Every possible measure should be taken to prevent recurrence and to improve patient survival. Patients diagnosed with this disease should be thoroughly counseled regarding its high risk of metastasis and recurrence, emphasizing the importance of long-term surveillance and regular follow-up. Olfactory esthesioneuroblastoma remains a rare entity, and its vague presenting symptoms often make early diagnosis challenging, resulting in most patients presenting at advanced stages of the disease. Advances in surgical and radiotherapy techniques over the past decade have significantly improved the prognosis of these tumors and, more importantly, reduced treatment- related toxicity.This case underscores the importance of early multidisciplinary management and vigilant long-term follow-up to ensure timely detection of recurrence in olfactory neuroblastoma.
Student And Decleration:
Ethical Approval: Not applicable
Competing Interests: None
Authors’ Contributions
Naima Amir: Wrote the manuscript
Zohaib Ahmed: Literature review
Muhammad Rafay: Critical revision of the manuscript.
Rabia Ali: Provide histology slides and description.
Funding: None
Availability Of Data And Materials
All data of the correspondence is publicly available on databases such as PubMed and Google scholar.
Informed Consent Statement
For the purpose of this case report, informed consent was obtained from the patient and her legal representative after a detailed discussion regarding the nature, purpose, and significance of the report. The patient was informed that her clinical details, including history, investigations, and management, would be shared in a dignified manner to protect her privacy. She was made aware that participation is voluntary, with no impact on the quality of care provided, and that while there is no direct benefit to her, the publication may contribute to medical knowledge and help other patients in the future. The patient understood the potential risks, including the minimal chance of loss of confidentiality due to the rarity of her condition, and voluntarily agreed to allow the use of her clinical information for publication and academic purposes.
References
- Mark S Greenberg (2023) Greenberg’s handbook of neurosurgery, US.
- Kuan EC, Nasser HB, Carey RM, Workman AD, Alonso JE, et al. (2018) A Population-Based Analysis of Nodal Metastases in Esthesioneuroblastomas of the Sinonasal Tract. Laryngoscope. 129(5): 1025-1029.
- AlQahtani DS, Alshamrani AA, AlQawahmed R, Elkhamary S, AlGhadeer H (2021) Olfactory Neuroblastoma: An Unusual Ocular Presentation. Neuor-opthalmology. 46(3): 182-185.
- Thomas J. Ow, Bell D, Kupferman ME, DeMonte F, Hanna EY (2017) Esthesioneuroblastoma. neurosurgery clinics of north america.
- Abdelmeguid AS, Bell D, Roberts D, Ferrarotto R, Phan J, et al. (2021) Long-Term Outcomes of Olfactory Neuroblastoma: MD Anderson Cancer Center Experience and Review of the Literature. Laryngoscope. 132(2): 290-297.
- Kumar A, Sethi B, Kumar Y, Mishra JP (2013) Esthesioneuroblastoma arising from the middle meatus. Journal of Cancer Research and Therapeutics. 9(1): 99-101.
- Jin Y, Zhang L, Qi W, Zhou Y, Kong J (2023) Olfactory neuroblastoma with rhabdomyoblasts: A rare case report and review of the literature. Indian J Pathol Microbiol. 66(2): 372- 374.
- Uslu GH, Canyilmaz E, Zengin AY, Mungan S, Yoney A, et al. (2015) Olfactory neuroblastoma: A case report. oncology letters. 10(6): 3651-3654.
- Aboziada MA, Eisbruch A (2010) Esthesioneuroblastoma: the role of post-operative irradiation after complete surgical resection. J Egypt Natl Canc Inst. 22(2): 143-8.
- Benfari G, Fusconi M, Ciofalo A, Gallo A, Altissimi G, et al. (2008) Radiotherapy alone for local tumour control in esthesioneuroblastoma. Acta Otorhinolaryngol Ital. 28(6): 292-7.
- McElroy EA Jr, Buckner JC, Lewis JE (1998) Chemotherapy for Advanced Esthesioneuroblastoma: The Mayo Clinic Experience. CNS Neurosurgery. 42(5): 1023-7
- Hoshi Y, Enokida T, Tamura S, Nakashima T, Okano S, et al. (2024) Efficacy of anti-PD-1 monotherapy for recurrent or metastatic olfactory neuroblastoma. Frontiers of oncology. 14: 1379013.