


Ratima Sood1, Taranjit Singh1, Shreya Gupta1, Rohit Bhatia2*
1Department of Pharmacy Practice, ISF College of Pharmacy Moga, Punjab, India-142001
2Department of Pharmaceutical Chemistry, ISF College of Pharmacy Moga, Punjab, India-142001
*Corresponding Author: Rohit Bhatia, Department of Pharmaceutical Chemistry, ISF College of Pharmacy Moga, Punjab, India-142001
Abstract
Splenomegaly is the pathological condition associated with enlargement of the spleen. It is generally caused by infections, cirrhosis, rheumatoid arthritis, various types of anemias, metabolic disorders, blood cancer, or autoimmune disorders. Splenomegaly leads to a variety of blood infections, modifications in the contents of blood constituents associated with several types of anemias. In the presented case report, we have detailed a 21 years old female patient who was suffering from anemic splenomegaly.
Introduction
Splenomegaly is outlined as enlargement of the spleen measured by weight or size. The “gold standard” defined splenomegaly by its weight: the normal spleen weighs 50-250g which lessens by age. This can be accepted at splenectomy or post mortem examination. The spleen plays a main role in hematopoiesis’s main functions of the spleen are clearance of senescent and abnormal erythrocytes, their remnants, opsonized platelets and WBC, and removal of microorganisms and antigens. The analytical findings of an observed spleen were antecedent to be proof of splenic enlargement but up to 16% of observed spleens are of normal size on radiological assessment [1,2]. Craniocaudal length is often used to observe splenic size; this corresponds with splenic volume, especially when the patient is laying down on the right side. A normal-sized spleen is 12 cm in craniocaudally length. A length between 12cm to 20 cm specifies splenomegaly and greater than 20 cm length demonstrates massive splenomegaly. An anteroposterior measure greater than two-thirds of the distance between the anterior and posterior abdominal wall is another ultrasonographic indicator of splenomegaly [3]. Complex formulae are used to evaluate splenic volume. Radiological endorsement of splenomegaly may therefore rely upon both radiologists’ preferred method and a degree of subjective judgment [4,5]. Anemia is a limiting factor in hemoglobin or hematocrit or RBC count. It is divided into microcytic, macrocytic, and normocytic.
Sign and Symptoms of Splenomegaly
In splenomegaly, Vague abdominal discomfort is the prime symptom. The clinical examination of a splenomegaly patient begins with a physical examination and through symptomatical history. Pressure effects from enlarged spleen including left hypochondria discomfort are observed. Few patients have also been found complaining about pain in the left shoulder. Distended abdomen, bloating and early satiety may also occur. Due to acute infections, the patient presents with fever, rigors, and weight loss. Symptoms of anemia such as dyspnoea, weakness may indicate splenomegaly due to an underlying hemolytic process. In patients with rheumatological diseases, the clinical features of splenomegaly include joint tenderness and swelling [6].
Pathophysiology
Remarkable enlargement in the mass of the spleen may result from a response to the change in the body’s normal physiology including blood loss and certain infections. Patients with non-cirrhotic portal hypertension may also present with splenomegaly and can result in serious complications such as variceal bleeding and ascites [7]. The enlargement is also observed as a result of chronic pathologies due to congestion or infiltration of the splenic environment. This type of enlargement is generally persistent and requires a specific therapy for its management. diseased cells resulting in based on pathophysiology, splenomegaly is classified as:
1. Congestive: It is secondary due to obstruction of blood flow in the splenic environment.
2. Infiltrative: Foreign cell invasion to the splenic environment leads to this type of splenomegaly.
3. Immune-mediated disorders
4. Neoplastic: It includes chronic lymphocytic leukemia and lymphoma [8].
Splenomegaly may be idiopathic or may be due to an underlying disease. On average, the normal human spleen is 10cm in length and 150g in weight. During splenomegaly, the weight may increase up to 2000g and length extending over 30cm. Splenomegaly ranges from mild to massive. It is considered massive in cases where the lower spleen pole is within the pelvis or it reaches beyond the midline. The pathophysiological mechanisms are broadly classified as Work Hypertrophy, Infiltration, or Congestion. Excessive splenic activities result in work hypertrophy. Enlargement of the spleen occurs due to sequestration of the abnormal erythrocytes from circulation. Diseases such as Sickle Cell Anaemia may cause engorgement of the venous sinus with diseased cells resulting in splenomegaly. Immune-mediated disorders including rheumatoid arthritis can result in follicular hyperplasia and can also affect the red pulp.
Infiltration can also promote splenic enlargement. The main infiltrates are lymphoma and primary myelofibrosis. In Gaucher disease, splenomegaly is a classic feature and the splenic size may increase up to 8-times the normal size due to the accumulation of lipids in splenic macrophages. The blockage of blood flow through the vasculature of the spleen can result in congestive splenomegaly and further lead to fibrosis of red pulp [9]. Figure 1 highlights the factors associated with anemic splenomegaly.
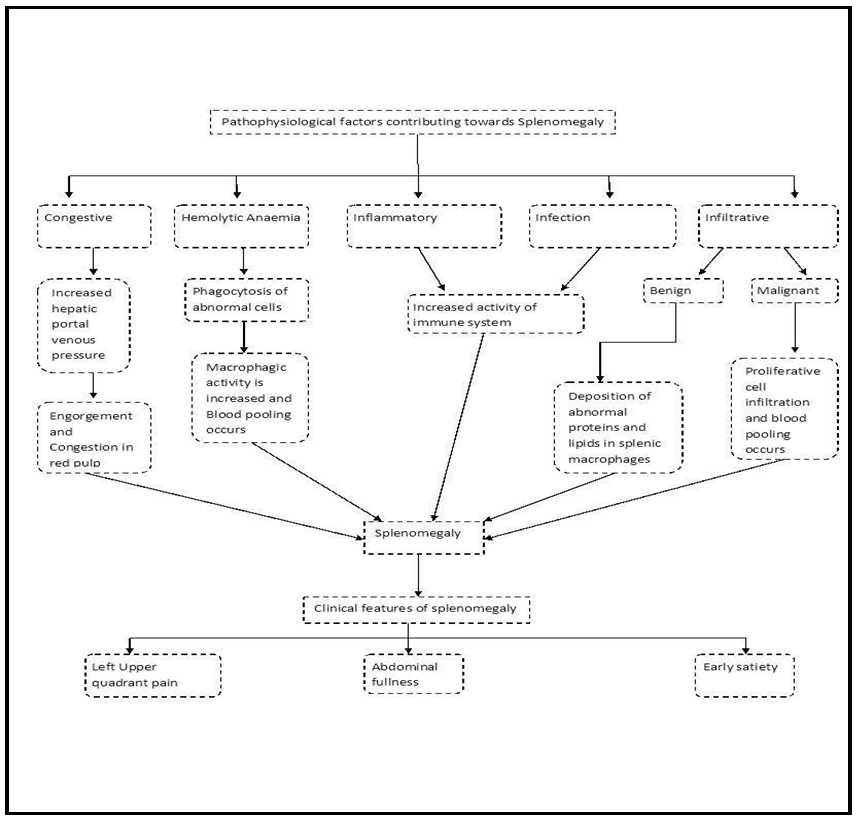
Figure 1: Factors associated with the pathophysiology of anemic splenomegaly
Case in detail
A 21-year-old female was hospitalized with chief complaints of bleeding gums from the last 2 days and yellow discoloration of eyes and urine for 25 days. She is a known case of Anaemia with some clinical symptoms of splenomegaly with manifestations of characteristics of easily fatigability, fever, and mildly increased pulse rate. The patient denied any history of decreased urine output or burning micturition. Furthermore, the patient denied any history of petechial or melena, pedal edema, bronchial asthma, diabetes mellitus, hypertension, COPD, and tuberculosis. There was no significant family history of any hematological disorder or anemia. But she was found to have jaundice 1 year back and 6 months before the referral date. Additionally, the patient was found to be vegetarian, non-alcoholic, and non-smoker. Besides, on examination, the patient was very calm, conscious, cooperative, as well as well oriented. Heart sounds were also normal. No additional murmuring was heard. Bowel and bladder habits were also normal. Table 1 presents the hematological report of the patient.
Table 1. Hematological report of the patient
|
Hematological parameters |
Patient’s value |
Normal value |
|
White blood cells |
4300/mm³ |
4500-11,000/mm³ |
|
Red blood cells |
2.6 million/mm³ |
Male – 4.3-5.9 million/mm³ Female – 3.5-5.5 million/mm³ |
|
Haemoglobin |
9.8g/dL |
Male – 13.5-17.5g/dL Female – 12.0-16.0g/dL |
|
Platelets |
143,000/mm³ |
150,000-4000, 000/mm³ |
|
MCV |
83mm³ |
80-100mm³ |
|
ESR |
70mm/hr |
0-20mm/hr |
CECT Report
Enlargement of spleen was shown which was about 15.5 cm but was homogenous. The portal vein and splenic vein were mildly dilated (14.0mm).
Impression: Anemia with splenomegaly.
Discussion
The patient was diagnosed with moderate splenomegaly and associated chief complaints were bleeding gums and discoloration of eyes and urine due to elevated ESR value. An abnormal increase in spleen size is generally due to multiple underlying factors that are blood disorders, decreased blood flow, cancer, and metabolic diseases such as Gaucher disease. Splenomegaly is one of the four fundamental signs of hypersplenism which includes a decrease in the number of erythrocytes. Enlargement of the spleen occurs when it performs more of its duties such as the formation of blood cells.
Eventually, any condition that damages red blood cells or anemia and requires them to be removed from the bloodstream will cause splenic enlargement. Currently, no medication can permanently cure our patient for splenomegaly. But injection Microfer and micro nerve forte were given to prevent and treat the low volume of iron and vitamin B12. If splenomegaly persists i.e the size of the spleen exceeds more than 20 cm, then in such cases patients are advised for surgical removal of spleen i.e splenectomy.
Treatment Strategies
At present the therapy options for splenomegaly are limited to the following options:
1. Symptomatic relief
2. Spleen reduction therapy
3. Splenectomy
In patients with primary myelofibrosis and hematological malignancies, spleen size is reduced using a low dose of radiation. In sickle cell anemia, splenic sequestration is treated with the help of blood transfusions. Patients who received partial splenectomy in Gaucher disease were found to regenerate the splenic tissues [10]. Surgical removal of the spleen i.e Splenectomy is the option for the chronic and critical cases of splenomegaly. Post-surgical antibiotic therapy is essential to minimize the possibility of infection.
Conclusion
Splenomegaly is associated with several abnormalities and anemia which may be lethal if left untreated. Therefore upon the appearance of the symptoms, it must be treated with a suitable treatment strategy.
References
- Chapman J, Bansal P, Goyal A, Azevedo AM (2021) Splenomegaly. StatPearls Publishing.
- Chow KU, Luxembourg B, Seifried E, Bonig H (2016) Spleen size is significantly influenced by body height and sex: establishment of normal values for spleen size at US with a cohort of 1200 healthy individuals. Radiology. 279(1): 306-313.
- Curovic Rotbain E, Lund Hansen D, Schaffalitzky de Muckadell O, Wibrand F, Meldgaard Lund A, et al. (2017) Splenomegaly– Diagnostic validity, work-up, and underlying causes. PLoS One. 12(11): e0186674.
- Olson AP, Trappey B, Wagner M, Newman M, Nixon LJ, et al. (2015) Point-of-care ultrasonography improves the diagnosis of splenomegaly in hospitalized patients. Critical ultrasound journal. 7(1): 13.
- Pozo AL, Godfrey EM, Bowles KM (2009) Splenomegaly: investigation, diagnosis and management. Blood reviews. 23(3): 105-111.
- Schloesser LL (1963) The diagnostic significance of splenomegaly. The American journal of the medical sciences. 245: 84-90.
- Nguyen Y, Stirnemann J, Belmatoug N (2019) Gaucher disease: A review. La Revue de medecine interne. 40(5): 313-322.
- McKenzie CV, Colonne CK, Yeo JH, Fraser ST (2018) Splenomegaly: Pathophysiological bases and therapeutic options. The international journal of biochemistry & cell biology. 94: 40-43.
- Freud E, Cohen IJ, Mor C, Golinsky D, Blumenfeld A, et al. (1998) Splenic “regeneration” after partial splenectomy for Gaucher disease: histological features. Blood Cells, Molecules, and Diseases. 24(3): 309-316.
- O'Keefe DA, Couto CG (1987) Fine‐needle aspiration of the spleen as an aid in the diagnosis of splenomegaly. Journal of veterinary internal medicine. 1(3): 102-109.