


Samima Batool1*, Ayesha Humayun1, Rabia Fatima2, Hafiza Asma Nazir1, Amna Idrees1, Jawaria Ghazanfar1
1Department of Public Health & Community Medicine, Shaikh Zayed Postgraduate Medical Institute, Lahore, Pakistan.
2Department of Chemical and Biomolecular Engineering, Clarkson University, Potsdam, New York, U.S.A.
*Corresponding Author: Samima Batool, Department of Public Health & Community Medicine, Shaikh Zayed Postgraduate Medical Institute, Lahore, Pakistan.
Abstract
Background: The threat of infant abductions and mix-ups in hospitals is a significant concern. While the United States has made strides in addressing this issue, Pakistan lacks comprehensive research and policies, resulting in a notable gap in evidence and policy implementation.
Objective: This study seeks to evaluate the readiness of public sector hospitals in Lahore, Pakistan, to prevent mother-baby mix-ups and abductions. It aims to assess hospital preparedness, factors influencing security, and maternal perceptions regarding this issue.
Methods: Employing a cross-sectional design, the study employed a modified questionnaire based on J. Rabun's hospital preparedness tool. The assessment covered 15 public sector hospitals in District Lahore, categorizing them as highly prepared, less prepared, or unprepared based on responses in four categories: General, Proactive Measures, Physical Security Safeguard, and Critical Incidence Response. Additionally, a list of 13 local factors was considered due to Pakistan's economic context. A semi-structured questionnaire was administered to 390 mothers to gauge their perceptions of baby abduction or mix-up risks and their satisfaction with security measures.
Results: The findings revealed that merely 2.85% of hospitals were categorized as highly prepared, while 11.43% showed low preparedness, and a substantial 85.72% were considered unprepared overall. Notably, practices such as informing mothers about newborn gender and using accurate tags for identification were widespread. However, having adequate guards per shift per ward needed to be improved in 80% of hospitals. Among surveyed mothers, 73.1% recognized the need for enhanced security, and 41.8% expressed concerns about potential incidents.
Conclusion: In conclusion, this study highlights a significant gap in the readiness of public sector hospitals in Lahore, Pakistan, to prevent mother-baby mix-ups and abductions.
Keywords: Infant abduction, Newborn kidnapping, newborn swiping, hospital security in developing countries, hospital security threats, public sector hospitals, hospital preparedness, maternal perceptions, risk factors, security analysis
Introduction
Healthcare facilities are vital in saving lives, providing emergency care, and aiding community recovery. However, the safety of hospitals faces numerous risks, especially concerning newborns, with incidents like abductions and mix-ups posing significant threats [3]. While cost-effective, traditional identification methods, such as written matching wristbands, have been linked to an increased risk of human error, leading to potential baby-mother mix-ups and abductions [8].
To address these challenges and ensure the utmost emergency preparedness, it is imperative to devise specific protocols utilizing advanced technologies like RFID systems and biometric verifications. [6].
Newborn abductions, characterized by non-family members taking infants under six months of age [2], and mix-ups, where babies are mistakenly handed over to the wrong parents, are issues of paramount concern for healthcare facilities [7]. The security of newborns, called neonatal security, becomes a fundamental aspect in assessing the quality of healthcare services [14].
Data from the National Center for Missing & Exploited Children (NCMEC) reveals the gravity of the situation, with 126 reported abduction cases in the USA between 1993 and 2006 [1]. Alarmingly, 43.46% of these incidents occurred within medical facilities, highlighting the need for improved security measures, especially within nursery units and mothers' rooms [4]. Newborn mother mix-ups occur approximately 23000 times each year in the USA, and according to research, the switching rate is 1 per 1000 infants [13].
The significance of this issue extends beyond borders, as developing countries, including Pakistan, face similar challenges due to insufficient security measures and easier access to nursery units. Even in Pakistan, 403 newborn abduction cases were reported in 2019 and 352 in 2020 in the Punjab province (CCPO office, Lahore). Investigating these cases is exceptionally challenging due to their rarity, complexity, involvement of high-profile individuals, emotional aspects, and lack of a comprehensive central record system (Ansari, 2019). In this study, we delve into the reasons behind such incidents in Pakistan's healthcare facilities, shedding light on the lack of awareness among hospital staff and administrative management gaps that contribute to the problem [17].
This article emphasizes the importance of considering mothers' perspectives to devise practical solutions for preventing newborn abductions and mix-ups. By understanding their experiences and concerns, healthcare providers can implement improved protocols and administrative strategies, creating a safer environment for newborns and instilling confidence in families and communities.
The objectives of this research are to evaluate the level of preparedness in public hospitals within District Lahore to avert cases of mother-baby mix-ups and abductions. It also aims to identify the underlying factors influencing such occurrences and to gauge the perspectives of mothers who have given birth in these hospitals regarding the possibilities of mix-ups and infant abductions.
Materials and Methods
Study Design: This cross-sectional study was conducted using a survey method to collect data from public sector tertiary and secondary level hospitals in District Lahore.
Sample Selection: The study included 12 tertiary and 3 secondary-level government sector hospitals in District Lahore. Key informants from each hospital, who were well-informed about the hospital's security measures, were selected to participate. Additionally, 390 mothers who delivered at these hospitals and were admitted to post-op wards or recovery rooms were interviewed.
Data Collection: Following institutional IRB approval, data collection was carried out through three questionnaires.
The first questionnaire, modified from NCMEC guidelines, covered hospital information and adherence to suggested guidelines across four categories: General, Proactive Measures, Physical Safeguard, and Critical Incidence Response.
The second questionnaire focused on local factors, assessing thirteen attributes with "Yes" or "No" responses for each hospital.
Lastly, a semi-structured Performa was used to gauge mothers' perceptions of hospital security, with five questions regarding fears of baby abduction or mix-up and satisfaction with facility security measures.
Statistical Analysis: Data collected from the questionnaires were entered into SPSS version 21 after appropriate coding. For the first questionnaire, hospitals were classified into three categories based on their responses to essential and recommended measures:
- Highly Prepared: Hospitals fulfilling 75-100% of the criteria for overall assessment.
- Low Prepared: Hospitals fulfilling 50-75% of the criteria for the general evaluation.
- Unprepared: Hospitals fulfill less than 50% of the criteria for the general evaluation.
Furthermore, the frequencies of each attribute from the second questionnaire and the responses from mothers in the third questionnaire were calculated to assess awareness levels and satisfaction regarding hospital security.
Results
Level of Hospital Preparedness: The study revealed that none of the hospitals qualified as "highly prepared" overall, with only one hospital (TR4) categorized as "highly prepared" in the general category. Across all categories (General, Proactive Measures, Physical Safeguard, and Critical Incidence Response), 85.72% of hospitals were deemed "unprepared." Only 2.85% of hospitals showed "low preparedness" in general guidelines, with a similar percentage in proactive measures (11.43%). Physical safeguard guidelines fared slightly better, with 20% of hospitals following the recommended steps. However, the critical incidence response category had the lowest adherence to essential guidelines at 15.7%.
Table 1: Summary table for all hospitals by categories:
|
Variables |
|
Highly Prepared |
Low prepared |
Unprepared |
|
General |
Essential Recommended |
03 ----- |
04 ---- |
08 ----- |
|
Proactive measures |
Essential Recommended |
00 00 |
00 01 |
15 14 |
|
Physical safeguard measures |
Essential Recommended |
00 00 |
01 06 |
14 09 |
|
Critical incidence response |
Essential Recommended |
00 00 |
00 00 |
15 15 |
|
Total |
(2.85%) |
(11.43%) |
85.72%) |
|
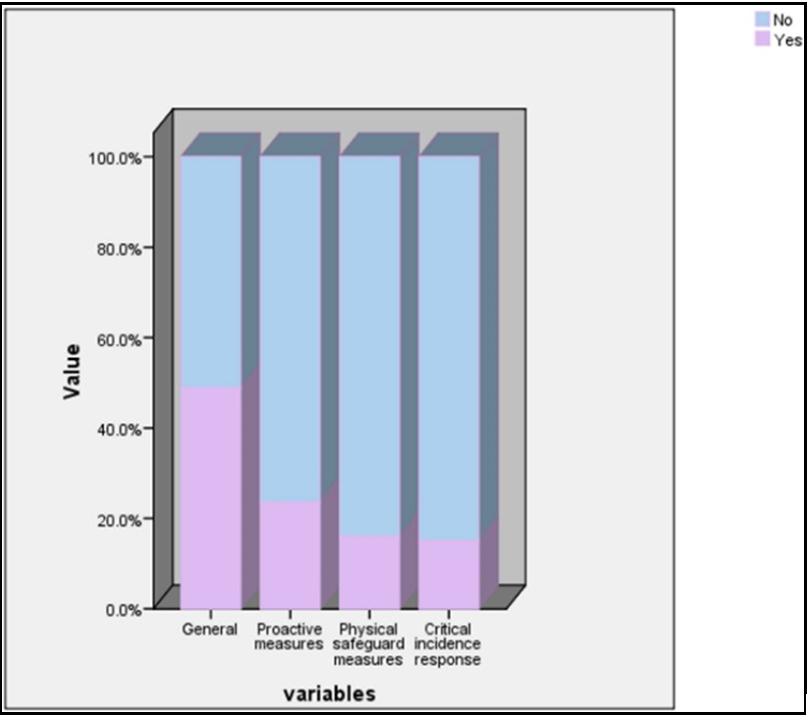
Figure 1: Graphical Presentation for Essential Guidelines (All Hospitals)
In short, the assessment revealed that none of the hospitals fell into the highly prepared category overall. Only one hospital exhibited high preparedness in the general category. Across all categories, only 2.85% of hospitals were highly prepared, while 11.43% were low prepared and 85.72% were unprepared. The graphical presentations depicted the distribution of essential and recommended guidelines followed by hospitals.
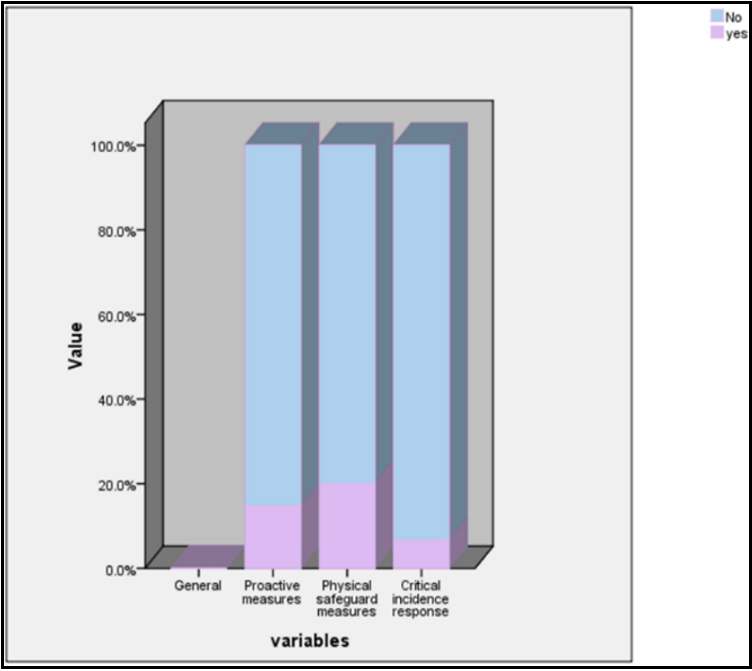
Figure 2: Graphical Presentation for Recommended Guidelines (All Hospitals)
Factors Adopted by Hospitals: The study highlighted specific measures adopted by hospitals to prevent newborn abductions and baby-mother mix-ups. Notably, all hospitals ensured that the mother was informed about the gender of the baby after birth, and tags with accurate information were simultaneously attached to the mother and baby. Additionally, all hospitals documented and supervised the baby's care effectively. However, other factors, such as having at least two guards per shift per ward and limiting births to one at a time, were less frequently implemented, with only 20% adherence.
Table 2: Frequency table for local factors of the hospitals:
|
Factors |
Yes |
No |
|
Same exit or entrance points |
8 (53.3%) |
7(46.7%) |
|
At least two guards per shift per ward |
3(20.0%) |
12(80.0%) |
|
One mother per bed |
6(40.0%) |
9(60.0%) |
|
Baby mothers are in same room |
8(53.3%) |
7(46.7%) |
|
One baby per cot/incubator |
5(33.3%) |
10(66.7%) |
|
Visiting hours are fixed |
7(46.7%) |
8(53.3%) |
|
Maximum two visitors allowed per mother |
7(46.7%) |
8(53.3%) |
|
Only one birth at one time |
3(20.0%) |
12(80.0%) |
|
Sufficient staff available |
9(60.0%) |
6(40.0%) |
|
Telling the mother about the gender of the baby right after birth |
15(100%) |
0(0.0%) |
|
Tag attached simultaneously to mother and baby with accurate information |
15(100%) |
0(0.0%) |
|
Tag was of good quality(undetectable) |
8(53.3%) |
7(46.7%) |
|
Baby receiving supervised and documented |
15(100%) |
0(0.0%) |
Maternal Perception: A substantial proportion (41.8%) of mothers believed there was a chance of infant abduction or mix-up at the facility. Although 49.7% had heard of such incidents, only 5.6% had personal experience with them. Encouragingly, 67.2% of mothers expressed satisfaction with the hospital's security measures. However, 73.1% of mothers believed there was a need for further improvement in security.
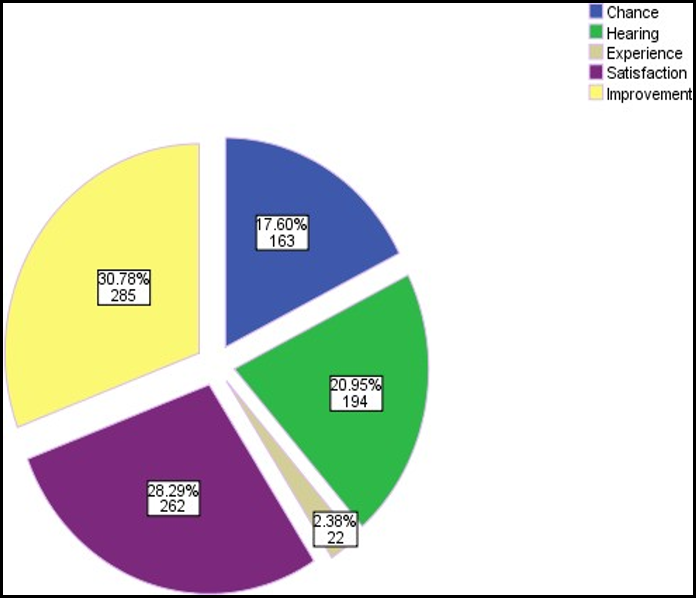
Figure 3: Graphical Presentation for the Perception of Mothers on the Subject Matter (Yes):
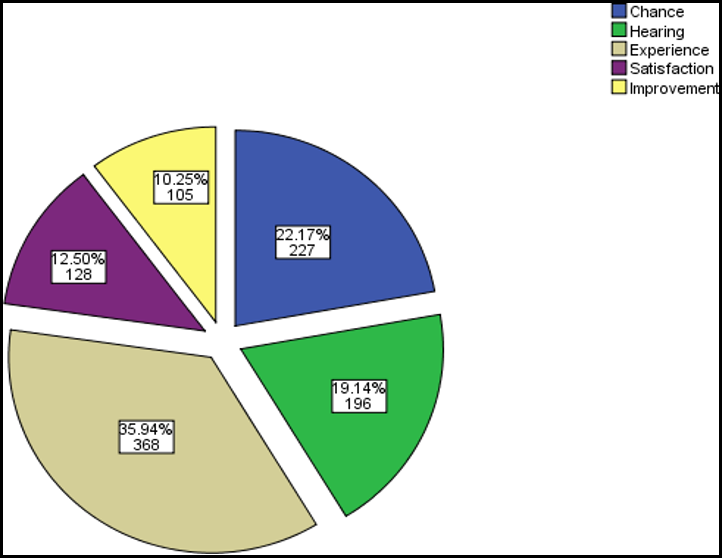
Figure 4: Graphical Presentation for the Perception of Mothers on the Subject Matter (No):
In conclusion, the analysis highlighted the need for enhanced hospital preparedness to prevent mother-baby mix-ups and abductions. While certain factors were being implemented effectively, there remained significant areas for improvement. Mothers' perceptions emphasized the importance of continuous efforts to ensure the safety and security of newborns and mothers in public hospitals.
Discussion
US hospitals actively enhance infant safety by treating misidentification and abduction as 'never' events, utilizing failure mode and effects analyses and robust action plans to prevent risks and strengthen security measures [15]. This study assessed hospital security preparedness for newborn abduction and mother-baby mix-ups in Pakistan, where rampant cases of infant abduction, with 403 reported in a year in Punjab, highlight an alarming situation (CCPO Office, Lahore). We evaluated public sector hospitals in Lahore using internationally accepted guidelines from NCMEC (a USA-based organization) to assess their preparedness for infant abductions [12]. The findings revealed that no hospital qualified as highly prepared, with TR4 being the most prepared in the general category. Only three out of 20 hospitals were considered highly prepared, 11.43% were rated as low-prepared, and a significant 85.72% were deemed unprepared, indicating a lack of readiness.
The study indicates that the critical incidence guidelines for abduction were poorly implemented in healthcare facilities, with no action plans observed. Despite the lack of reported abductions after implementing postpartum floor lockdowns, maintaining and improving safety protocols is crucial to address potential loopholes and human factors and ensure ongoing protection for vulnerable newborns. Complacency should be avoided; newborn safety remains a top priority [9].
Traditional methods for newborn identification in Pakistani healthcare facilities are still predominantly used, highlighting the need for technological integration to enhance security measures [5]. While practices like sharing the baby's gender with the mother and using matching tags for mothers and babies have been adopted in all hospitals, research indicates that alternative distinct naming strategies do not significantly reduce wrong-patient ordering errors. Addressing patient misidentification requires further measures to reduce the mistakes related to a small percentage of clinicians [11].
This study emphasizes the importance of understanding mothers' perspectives on newborn identification issues to provide healthcare providers with valuable insights and address the severe psychological effects of mother-baby mix-ups, where individuals express a desire to reconnect with their biological parents because they feel disconnected from their true origins [16].
This study focused on the perspectives of mothers who gave birth at government hospitals regarding newborn abduction and safety arrangements. The findings revealed that 41.8% of mothers expressed concerns about the lack of a biometric system in hospitals. While 67.2% were satisfied with existing security measures, the majority (73%) believed there was substantial room for improvement, highlighting the need for attention and resources to enhance patient safety and risk reduction in obstetricians.
Essential suggestions involving clinical knowledge, bias, racism, individualized care, communication training, and personalized solutions are necessary for enhancing women's and families' health, requiring ongoing dialogue and collaboration among healthcare professionals to achieve better outcomes for mothers and newborns [10].
This research calls for further investigations, encompassing private hospitals and different regions of Pakistan, to comprehensively understand newborn abduction and mix-up issues. It emphasizes the significance of studying the perspectives of hospital staff, exploring root causes, and comparing practices with developed countries to implement targeted interventions and enhance hospital security for newborns' protection. Overall, the study highlights the urgent need for improved security measures, stricter protocols, and increased awareness to address these alarming issues effectively.
Conclusion
In conclusion, this study assessed the readiness of public sector hospitals in Lahore, Pakistan, to prevent mother-baby mix-ups and abductions. The findings revealed a significant gap in hospital preparedness. While certain measures, such as informing mothers about newborn gender and using accurate tags for identification, were widespread, other critical factors, such as having adequate guards per shift per ward, were deficient in most of the hospitals. Among surveyed mothers, the maximum number of mothers recognized the need for enhanced security and expressed concerns about potential incidents. This study highlights the need for further research and investigations in other regions of Pakistan, including private hospitals, to comprehensively understand the issue. Comparative studies with developed countries can also provide valuable insights into best practices and strategies for preventing mother-baby mix-ups and abductions. In conclusion, addressing the issue of mother-baby mix-ups and abductions requires a multi-faceted approach that includes the implementation of advanced technologies, the development of comprehensive protocols, staff training and education, and active engagement with mothers. By taking these steps, public sector hospitals in Lahore, Pakistan, can improve their readiness and ensure the safety and security of newborns and their mothers.
References
- Burgess AW, Carr KE, Nahirny C, Rabun JB Jr (2008) Nonfamily infant abductions, 1983– 2006. AJN The American Journal of Nursing. 108(9): 32-38.
- Cesario SK (2003) Selecting an infant security system. AWHONNlifelines. 7(3): 236-242.
- Dizdarević A, Ovčina A, Ramić A (2022) Determination of hospital security index for emergenciesand evaluation indicators. Sestrinski glasnik. 27: 175-181.
- Jaronde PW, Muratkar NA, Bhoyar PP, Gaikwad SJ, Nagrale RB (2018) Review on biometric security system for newborn baby. International Journal of Scientific Research in Science and Technology. 4(2): 907-909.
- Jhaveri H, Jhaveri H, Sanghavi D (2014) Biometric security system and its applications inhealthcare. International Journal of Technical Research and Applications. 2(6): 15-20.
- Jung YG, Kang JS (2011) Hospital Security System using Biometric Technology. The Journal of The Institute of Internet, Broadcasting and Communication. 11: 219-224.
- Lalović K, Maček N, Milosavljević M, Veinović M, Franc I, et al. (2016) Biometric verification of maternity and identity switch prevention in maternity wards. Acta Polytechnica Hungarica. 13(5): 65-81.
- Lin L, Yu N, Wang T, Zhan C (2011) Active rfid based infant security system. Communication Systems and Information Technology. Springer. 203-209.
- Neshek B, Bryant DR, Hruska J, Gupta D (2023) The Impact of Peripartum Floor Lockdowns onNewborn Safety. medRxiv. 28: 23289274.
- OʼNeill L, Miller LA, Rohan AJ (2020) Threats to patient safety in the inpatient maternitysetting. MCN: The American Journal of Maternal/Child Nursing. 45(2): 74-81.
- Pfeifer E, Lozovatsky M, Abraham J, Kannampallil T (2020) Effect of an alternative newbornnaming strategy on wrong-patient errors: a quasi-experimental study. Applied clinical informatics. 11(2): 235-241.
- Rabun JB (2009) For healthcare professionals: Guidelines on prevention of and response to infantabductions. National Center for Missing & Exploited Children.
- Rizk K, Kayle M, Mekawi L. Prevention of Infant Abductions and Mix-ups in Hospitals.
- Smith AD (2009) Marketing and reputation aspects of neonatal safeguards and hospital-security systems. Health Marketing Quarterly. 26(2): 117-144.
- Webster KLW, Stikes R, Bunnell L, Gardner A, Petruska S (2021) Application of human factors methods to ensure appropriate infant identification and abduction prevention within thehospital setting. The Journal of Perinatal & Neonatal Nursing. 35(3): 258- 265.
- Welner M, Burgess A, O'Malley KY (2021) Psychiatric and legal considerations in cases of Fetal Abduction by Maternal Evisceration. Journal of forensic sciences. 66(5): 1805-1817.
- Ashraf Javed (2008) Police fail to find missing newborn. The Nation.