


Alebtekin Ahangari PT, MPH
Rehabilitation Dean, Golestan Welfare Administration, Gorgan, Golestan province, Iran
Abstract
Context
Spinal Cord Injury is accompanying by numerous changes in a person’s life. Besides surgical and pharmacological interventions, enabling individuals with SCI is possible through rehabilitation programs. The paradigm of rehabilitation and physiotherapy for this group has changed from medical aspects to notions including participation and quality of life which can be achieved through routine exercise and assistive devices. Many of the approaches and assistive technologies especially for standing and gait training are expensive and are not available for many individuals with SCI in different societies. Therefore, easy to reach and inexpensive interventions could increase individuals’ abilities and facilitate reaching the goal of interventions including participation and empowerment.
Findings
The patient was 59-year-old women who were injured in an accident suffered a fracture of both luminar base as well as the spinous process of C7 with partial collapse and fracture of the anterior aspect of a vertebral body with partial collapse and overriding anterior dislocation C6 over C7 in cervical spine CT scan. The patient was grade A on ASIA-Scale and her SCIM-Scale V. III was 10.
Conclusion
This case report tried to present the possibility of increasing cervical SCI patient’s abilities by introducing inexpensive home-made adjustment instruments to perform daily living activities and standing exercises even without hard to access and expensive standing devices.
Keywords: rehabilitation, integration, participation, spinal cord injury, the activity of daily living.
Introduction
Spinal Cord Injury [1] with 15-40 cases/million in developed countries [1], is accompanying by numerous changes in a person’s life [2-6] and may have complications including respiratory problems, [7] sores [2,3], and marginalization [3] in addition to the economic burden on individuals and their family [6,8]. Traumatic SCI has more complications with a higher probability of mortality [3]. With keeping in mind the notion of the possible capacity of neural regeneration also incomplete SCI, besides surgical and pharmacological interventions [4], enabling individuals with SCI is possible through rehabilitation programs [3,4,9] and removing barriers such as mobility skills [10] which provide and enhance individuals abilities to overcome different types of barriers and finally, increase participation. [3, 5, 10] Increasing muscle strength in SCI individuals is challenging which can be done in different ways [11] but the cost and access are doubtful. Therefore, many cases of individuals with SCI have a weak muscle strength and secondary complications. Through interventions, it is possible to change SCI grade on American Spinal Injury Association Scale (ASIA- Scale) [4,12]. Paradigm of rehabilitation and physiotherapy has changed for these group from medical aspects to notions including participation and quality of life which can be achieved through routine exercise and assistive devices. [10] Predicting factors of the amount of Activity of Daily Living (ADL) recovery in cervical SCI are including age, level of injury, and severity. [9] For individuals with cervical SCI, in addition to lower extremity, arms and hands dysfunction occurs, therefore rehabilitation to bring their function become their priority [13,14]. Many of the approaches and assistive technologies especially for standing and gait training are expensive and are not available for many individuals with SCI in different societies. Therefore, having easy to reach and inexpensive interventions could increase individuals’ abilities and facilitate reaching the goal of interventions including participation and empowerment.
Case Report
The patient was 59 years old women at the accident date who suffered a fracture of both luminar base as well as the spinous process of C7 with partial collapse and fracture of the anterior aspect of the vertebral body with partial collapse and overriding anterior dislocation C6 over C7 in cervical spine CT scan (Figure 1).

Figure 1: The first cervical spine CT-scan after trauma.
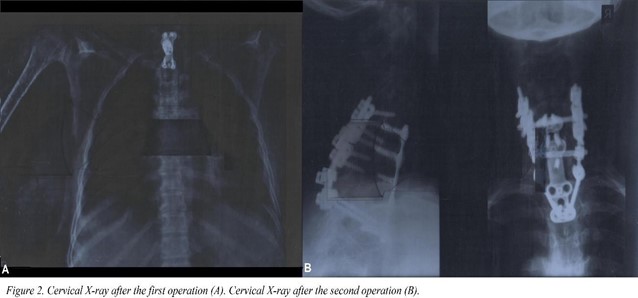
She underwent C5-T1 fixation operation by nail and plaque (Figure 2-A). The patient was grade A on ASIA-Scale and her Spinal Cord Independence Measure V. III (SCIM) was 10 (Table 1).
Table 1: Spinal Cord Independence Measure V. III
|
Domain |
First month |
Three months |
Six months |
12 months |
18 months |
24 months |
|
Self-care |
0 |
0 |
0 |
3 |
5 |
6 |
|
Respiration and Sphincter Management |
10 |
10 |
10 |
10 |
10 |
10 |
|
Mobility (room and toilet) |
0 |
0 |
0 |
2 |
2 |
2 |
|
Mobility (Indoors and Outdoors, on even surfaces) |
0 |
0 |
1 |
2 |
2 |
2 |
Physiotherapy intervention was implemented immediately after discharge from hospital to home including passive range of motion and electrotherapy. Two months after the first operation and following the loosening of fixation without any medical complications, the patient had hospitalized to have a second operation of C7-T1 corpectomy and C6-T2 fixation (Figure 2-B).
Physiotherapy program was continued at home, as well as previous procedures including isometric exercises of the shoulder girdle, sitting with support and weight-bearing on upper extremities, and active- assisted range of motion. She had 23 days of admission at a special rehabilitation hospital eight months after the second operation. Following discharge from the rehabilitation hospital, more active exercises were included in the physiotherapy program. Since standing training equipment such as tilt table is expensive and very few to reach and on the other hand, assistive devices such as different types of braces are not easy to use especially in the first month’s post-trauma, after strength, equilibrium, respiratory, and proprioception training in different positions, standing training with walker and positioning therapist in front of the patient begun (Figure 3). The first difficulty was low cardiopulmonary endurance in addition to incoordination between therapist and patient. The second was a requirement of a third person to help in sitting to standing transition. After one week of training, the later problems ratified and then focus was on increasing patient standing endurance (Figure 3).
Figure 3: Standing position.
To encourage patient to use their upper extremity and facilitating the integration of the individual into the family, a home-made assistive device to hold eating instruments prepared by the family were introduced (Figure 4).

Figure 4: Example of home-made assistive device.
These two interventions increased patient abilities on the SCIM scale (Table. 1) but ASIA-Scale remained the same. This progress prominently was in the self-care domain (from zero in the first month to six in the 24th months).
Discussion
This is a case report of women with traumatic cervical SCI with the aim to present the usefulness of integrating simple assistive devices and personal aid to improve patient abilities and social integration. Even though in many cases, cervical SCI patient mostly undergoes rehabilitation of upper extremity and standing exercises missed, this case report tried to present the possibility of increasing cervical SCI patients’ abilities by introducing inexpensive home-made adjustment instruments to perform daily living activities and standing exercises even without hard to access and expensive standing devices.
Conclusion
The rapists and families of cervical SCI have challenges to provide instruments and devices to train and help patients to become more independent. Despite this fact, there are easy and inexpensive methods and home-made to achieve independence which therapists and families could use.
Acknowledgment: None
Funding: None
Disclaimer Statements: None
Declaration of interest: The author declares no potential conflict of interest.
References
- Mingaila S, Krisciunas A (2004) [Occupational therapy in spinal cord injury]. Medicina. 40(8): 816-9.
- Gelis A, Stefan A, Colin D, Albert T, Gault D, et al. (2011) Therapeutic education in persons with spinal cord injury: a review of the literature. Annals of physical and rehabilitation medicine 54(3): 189-210.
- Kashif M, Jones S, Darain H, Iram H, Raqib A, et al. (2019) Factors influencing the community integration of patients following traumatic spinal cord injury: a systematic review. J Pak Med Assoc. 69(9): 1337-1343.
- Gomes-Osman J, Cortes M, Guest J, Pascual-Leone A (2016) A Systematic Review of Experimental Strategies Aimed at Improving Motor Function after Acute and Chronic Spinal Cord Injury. Journal of neurotrauma 33(5): 425-38.
- Tomaschek R, Gemperli A, Rupp R, Geng V, Scheel-Sailer A, et al. (2019) A systematic review of outcome measures in initial rehabilitation of individuals with newly acquired spinal cord injury: providing evidence for clinical practice guidelines. European journal of physical and rehabilitation medicine 55(5): 605-617.
- Ahuja CS, Schroeder GD, Vaccaro AR, Fehlings MG (2017) Spinal Cord Injury-What Are the Controversies? Journal of orthopaedic trauma 31(Suppl 4): S7-S13.
- Ushiku C, Suda K, Matsumoto S, Komatsu M, Takahata M, et al. (2019) Time Course of Respiratory Dysfunction and Motor Paralysis for 12 Weeks in Cervical Spinal Cord Injury without Bone Injury. Spine surgery and related research 3(1): 37-42.
- Cadotte DW, Fehlings MG (2011) Spinal cord injury: a systematic review of current treatment options. Clinical orthopaedics and related research 469(3): 732-741.
- Wirz M, Dietz V (2015) Recovery of sensorimotor function and activities of daily living after cervical spinal cord injury: the influence of age. Journal of neurotrauma 32(3): 194-9.
- Gomara-Toldra N, Sliwinski M, Dijkers MP (2014) Physical therapy after spinal cord injury: a systematic review of treatments focused on participation. The journal of spinal cord medicine 37(4): 371-9.
- de Freitas GR, Szpoganicz C, Ilha J (2018) Does Neuromuscular Electrical Stimulation Therapy Increase Voluntary Muscle Strength After Spinal Cord Injury? A Systematic Review. Top Spinal Cord Inj Rehabil. 24(1): 6-17.
- AlHuthaifi F, Krzak J, Hanke T, Vogel LC (2017) Predictors of functional outcomes in adults with traumatic spinal cord injury following inpatient rehabilitation: A systematic review. J Spinal Cord Med. 40(3): 282-294.
- Spooren AI, Janssen-Potten YJ, Kerckhofs E, Seelen HA (2009) Outcome of motor training programmes on arm and hand functioning in patients with cervical spinal cord injury according to different levels of the ICF: a systematic review. J Rehabil Med. 41(7): 497-505.
- de los Reyes-Guzman A, Gil-Agudo A, Penasco-Martin B, Solis- Mozos M, del Ama-Espinosa A, et al. (2010) Kinematic analysis of the daily activity of drinking from a glass in a population with cervical spinal cord injury. Journal of neuroengineering and rehabilitation 7: 41.