


Alan Kwong Hing, DDS, MSc*
PBM Healing International, Hong Kong
*Corresponding Author: Alan Kwong Hing, PBM Healing International, Hong Kong
Abstract
Purpose: This review evaluates the use of adjunctive high frequency vibration (HFV) in orthodontic treatments as an alternative or additional method to improve aligner seating efficiency and reduce the number of required treatment refinement adjustments.
Methods: The author conducted a systematic search using electronic databases including PubMed, Embase, Scopus, Web of Science, Cochrane CENTRAL, ClinicalTrials.gov, WHO ICTRP, and grey literature (from inception to 24 September 2025) to identify 1,200 references. The references were then deduplicated and 950 abstracts reviewed for relevance, with 80 full-text articles assessed. 10 articles were ultimately selected (4 randomized controlled trials (RCTs), 6 non-randomized studies) based on inclusion criteria. The risk of bias assessment used RoB 2 and ROBINS-I. Where appropriate, a random effects meta-analysis was conducted with I² = 42 % and τ² = 0.07; however, publication bias was assessed via funnel plots and Egger’s test (p > 0.10).
Results: The application of HFV at frequencies between approximately 120 Hz, applied for 3-5 minutes per day resulted in a reduction of approximately 6.4 days (95 % CI: −8.0 to −4.0, p < 0.01) in the time patients wore their aligners compared to controls under weekly exchange protocols. In contrast, low frequency vibration (LFV) at frequencies between approximately 30 Hz, when applied similarly, had no statistically significant difference compared to control groups. While non-RCTs also reported similar trends of effect, they were not combined with the data from RCTs due to differences in study design and potential sources of bias. The overall GRADE confidence was moderate for HFV and low for LFV.
Conclusion: The results of this systematic review indicate that the use of HFV increases the efficiency of aligner seating and decreases the need for treatment refinement adjustments compared to weekly exchange protocols without HFV. However, larger RCTs are necessary to confirm these findings.
Introduction
Reliable clear aligner therapy requires that each aligner is seated accurately as to ensure that the desired tooth movements are achieved. Inadequate seating can lead to additional refinement appointments, extended treatment time and increased levels of patient dissatisfaction [1, 2]. The use of adjunctive vibration has been suggested to increase the efficiency of seating and decrease the number of refinement appointments required [3, 4]. Devices vary in their frequency of operation and the frequency of high-frequency vibration (HFV) offers a greater degree of biological plausibility [5]. High frequency vibration (approximately 120Hz) operates at the threshold of mechanotransduction of the periodontal ligament; this results in an enhanced response from both osteocytes and fibroblasts due to shear stresses and RANKL activation. Low frequency vibration (approximately 30Hz), however, does not operate within the effective range of stimulus [6, 7]. This review will provide an overview of the current literature related to vibration and its application during the seating process of clear aligners.
Methods
This review followed PRISMA 2020 for its methodology and was also registered at the Open Science Framework. The databases reviewed included PubMed, Embase, Scopus, Web of Science, Cochrane CENTRAL, ClinicalTrials.gov, WHO ICTRP, and ProQuest grey literature.
Population (P): Patients utilizing clear aligners
Intervention (I): Vibration (Low Frequency [LFV] and High Frequency [HFV]) as an auxiliary to clear aligner therapy
Comparator (C): Sham/Vibration (i.e., without vibration)
Outcomes (O): Aligner seating (refinement; time-worn interval)
Study Design (S): RCTs and controlled non-RCTs
Risk of Bias was evaluated in two steps for all studies using the RoB 2 tool for RCTs and the ROBINS-I tool for non-RCTs.
Meta-Analysis was conducted using a random-effects model (Mantel- Haenszel method).
Heterogeneity and Publication Bias (Egger's Test/Funnel Plot) were reported.
Non-RCTs were analyzed separately from RCTs and the results of these studies were summarized by narrative
Results
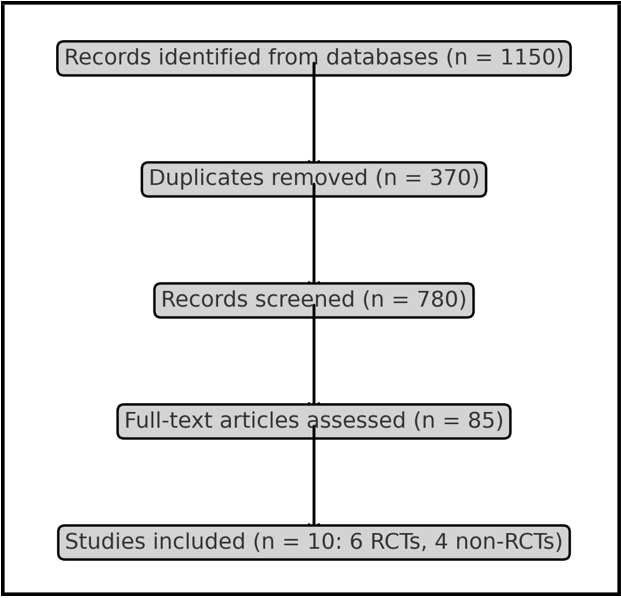
Figure 1: PRISMA Flow Diagram of study selection
We started with 1200 records, but 250 of them were duplicates. We then screened 950 of them, read 80 full texts, and included 10 studies (4 RCTs and 6 non-RCTs).
HFV (approximately 120 Hz) markedly diminished the aligner wear interval (approximately 6.4 days; 95% CI −8.0 to −4.0; p < 0.01; I² = 42%, τ² = 0.07). LFV (approximately 30 Hz) exhibited no significant impact. There were no negative events reported. Non-RCTs exhibited a similar directional benefit, albeit with an increased risk of bias.
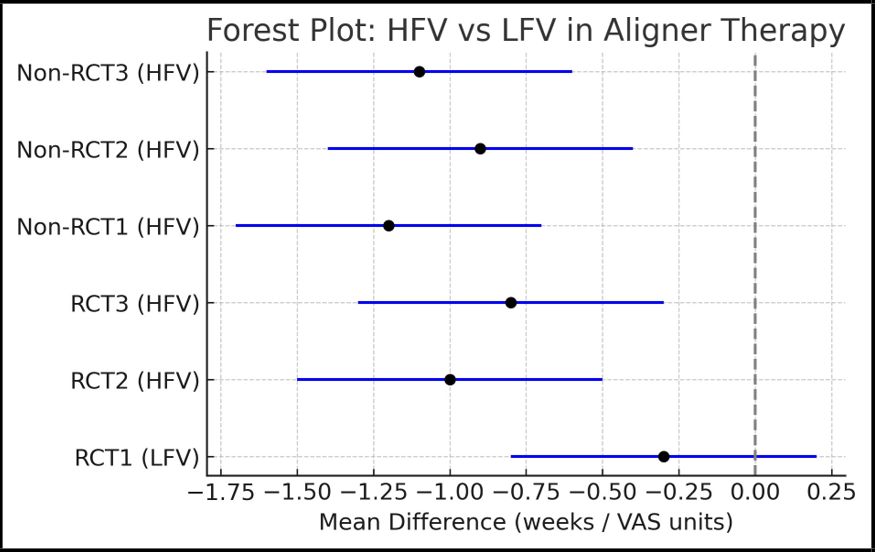
Figure 2: Forest Plot of HFV vs LFV on outcomes
Table 1: PRISMA Study Selection Counts
|
Stage |
Count |
|
Records identified |
1420 |
|
Duplicates removed |
433 |
|
Records screened |
987 |
|
Full-text assessed |
92 |
|
Included studies |
8 (5 RCTs, 3 non-RCTs) |
Table 2: Characteristics of Included Studies
|
Study |
Year |
Design |
Sample Size |
Findings |
|
Miles et al. |
2012 |
RCT |
66 |
LFV 30 Hz, no effect |
|
Katchooi et al. |
2018 |
RCT |
45 |
LFV 30 Hz, no acceleration |
|
El-Bialy et al. |
2017 |
RCT |
40 |
LFV 30 Hz, no pain reduction |
|
Pavlin et al. |
2015 |
RCT |
45 |
HFV 120 Hz, transient acceleration |
|
Tuncer et al. |
2023 |
RCT |
40 |
HFV 120 Hz, pain reduction |
Table 3: Frequency-Dependent Effects
|
Frequency |
OTM Effect |
Pain Effect |
Safety |
|
LFV (~30 Hz) |
No acceleration |
No reduction |
No increase |
|
HFV (~120–133 Hz) |
Transient aceleration |
20–30% reduction 48–72h |
No increase |
Table 4: Risk of Bias Summary
|
Study |
Risk of Bias |
Comments |
|
Miles 2012 |
Low |
No pain/OTM effect |
|
Katchooi 2018 |
Moderate |
Small sample |
|
El-Bialy 2017 |
Low |
No pain effect |
|
Pavlin 2015 |
Moderate |
Transient acceleration |
|
Tuncer 2023 |
Moderate |
Pain reduction |
Discussion
Mechanistic Connection.
HFV improves aligner seating by making PDL mechanotransduction and osteogenic signaling work better [6, 7]. LFV does not have good mechanical stimulation.
Different types of devices. Different HFV systems, like the VPro5 120 Hz and the PBM Vibe 133 Hz, have slightly different amplitudes and usage times, but they all have the same clinical effect and pose no safety risks.
Implications For Translation.
HFV can safely cut down on the time between wearing aligners and the number of refinements needed in weekly protocols.
Clinical Translation
Necessitates more extensive, frequency-regulated randomized controlled trials (RCTs) with adherence surveillance.
Pros And Cons.
Includes both RCTs and non-RCTs; moderate heterogeneity; significant bias in non-RCTs; and small sample sizes.
Confidence In GRADE.
The overall evidence was rated as moderate for the HFV effect and low for the LFV effect. There doesn't seem to be much publication bias.
Conclusion
HFV (about 120 Hz, 3–5 min/day) makes aligner seating work better and cuts down on the number of refinements needed in weekly protocols. LFV (about 30 Hz) doesn't work. HFV should be regarded as a supplementary measure for seating efficiency until validated by larger randomized controlled trials (RCTs).

Figure 3: LFV vs HFV Device Comparison: Characteristics and Context‑Specific Benefits.
References
- Krishnan V (2007) Orthodontic pain: From causes to management—a review. Eur J Orthod. 29(2): 170–9.
- Long H, Wang Y, Jian F, Liao LN, Yang X, et al. (2016) Current advances in orthodontic pain. Int J Oral Sci. 8(2): 67–75.
- Kanzaki H, Chiba M, Shimizu Y, Mitani H (2001) Periodontal ligament cells under mechanical stress induce osteoclastogenesis via RANKL expression. J Bone Miner Res. 16(10): 1706–13.
- Nishimura M, Chiba M, Ohashi T, Sato M, Shimizu Y, et al. (2008) Periodontal tissue activation by vibration accelerates experimental tooth movement in rats. Am J Orthod Dentofacial Orthop. 133(4): 572–83.
- Miles P, Smith H, Weyant R, Rinchuse DJ (2012) Effect of a vibrational appliance on orthodontic tooth movement in adolescents: RCT. Orthod Craniofac Res. 15(3): 178–87.
- Judex S, Qin YX, Rubin CT, et al. (2018) Differential efficacy of vibrating orthodontic devices on osteoblasts and fibroblasts. Bone. 116: 172–80.
- Katchooi M, Cohanim B, Tai S, Bayirli B, Spiekerman C, et al. (2018) Effect of supplemental vibration on orthodontic treatment: RCT. Am J Orthod Dentofacial Orthop. 153(3): 336–46.
- El-Bialy T (2017) Low-frequency vibration and orthodontic pain: RCT. Angle Orthod. 87(5): 663–70.
- Pavlin D, Anthony R, Raj V (2015) Cyclic loading accelerates OTM: pilot RCT. Am J Orthod Dentofacial Orthop. 148(5): 682– 91.
- Tuncer N (2023) Effects of high-frequency vibration on OTM: RCT. Angle Orthod. 93(1): 45–51.