


Anna Susan Paul1*, CR Saju2, Sruthi MV3, Tharun C Varghese4, Jini MP5
1Public Health Specialist, Airport Health Organization, Cochin International Airport, Kerala
2Professor and HOD, Department of Community Medicine, Amala Institute of Medical Sciences, Thrissur
3Assistant Professor, Department of Community Medicine, Amala Institute of Medical Sciences, Thrissur
4Junior Consultant,Paediatrics,Apollo Adlux hospital, Angamaly.
5Biostatistician, Department of Community Medicine, Amala Institute of Medical Sciences, Thrissur
*Corresponding Author: Anna Susan Paul, Public Health Specialist, Airport Health Organization, Cochin International Airport, Kerala.
Abstract
Adolescence is a period of great physical and psychological transition. Parents play an essential role in providing a comfortable environment for Sexual and Reproductive Health (SRH) information for adolescents during this period. This study was conducted to assess the sexual and reproductive health communication between adolescent high school students and their parents in the Thrissur district and determine the facilitating factors and barriers. A cross-sectional study was conducted among adolescent high school students in Thrissur district, Kerala, from December 2019 to May 2021. A multistage sampling technique was used, and a sample size 338 was achieved. Data was collected using a self-administered questionnaire. Statistical analysis included descriptive statistics, chi-square test, Fisher's Exact test, and binary logistic regression. The mean age of the study population was 14.2 ± 0.88 years, and 58 % were females. The majority had average SRH communication [179 (53 %)]. Only 67 (19.8 %) adolescents had good SRH communication. The majority had a strong positive attitude towards SRH communication with parents [140 (41.4 %)]. The feeling of shame, cultural unacceptability, and lack of communication skills in parents were perceived as significant barriers to communication. Bivariate analysis showed a statistically significant association between SRH communication and adolescents' gender, the number of females and males at home, and a positive attitude towards SRH communication (p < 0.05). Binary logistic regression analysis showed that the odds of having good SRH communication was 1.206(0.65-2.21) times more for females than males. More number of females at home was a factor for good SRH communication with an odds of 1.23(0.83-1.81), while a smaller number of males at home favored good communication [OR:0.91(0.611.35)].
Keywords: Adolescents, Parents, Sex education, Sexual and Reproductive health (SRH) Communication.
Introduction
The world now has more young people than ever before. WHO defines 'young' as those aged between 10-24 years and those aged 10- 19 years as' adolescent.' [1] Adolescence is a time of opportunity for exploration, and they are not free from behavior patterns that may risk their current and future health.[2] It is a critical and challenging period when people become independent individuals, forge new relationships, develop new social skills, and learn behaviors that will last their lives. Of the 7.2 billion people worldwide, over 3 billion are younger than 25 (42 % of the world population). Around 1.2 billion of these young people are adolescents.[1] Nearly one-third of India's population is 10–24 years old.[3] In this rapid neurological, physical, and emotional transition from childhood to adulthood, young people face a range of health risks. They face sexual health issues such as Sexually Transmitted Infections (STIs), sexual exploitation, teenage pregnancy, etc. [1] The global fertility rate of adolescents aged 15-19 is 50 births /1000 women.[4] Ideals about body image, glorification of alcoholism in media, social exclusion, detachment from parents, rapid physiological and neurological changes, and the urge for exploration and experimentation make it hard for them to cope with the various challenges. Many young people experience risky sexual activity, do not receive appropriate care, and experience adverse reproductive health outcomes. Over 35 % of all reported HIV infections in India occur among young people 15–24.[5]. Every year, 2.5–3 million adolescents globally acquire STIs. This implies that approximately one out of every ten adolescents acquire STIs yearly, even in developed countries. Over one million teenagers become pregnant yearly, of which 60 % are unwanted pregnancies resulting from unprotected sex.[6] Globally, about 1 in 10 girls under 20 have been subjected to forced sexual acts at some point. 90 % of adolescent girls who reported exploitation say that their first abuser was someone known to them, usually a boyfriend or a relative. Globally, more than a quarter of adolescent girls aged 15–19 have been the victims of emotional, physical, or sexual violence at some point.[7] Most children do not report these to their parents due to inadequate communication skills or a lack of healthy relationships. Today, over one billion 10–19-year-olds, 70 %, live in developing countries. They grow up in circumstances quite different from their parents, with greater access to formal education, an increasing need for technological skills like internet literacy, and exposure to new ideas through media, telecommunications, etc. The Covid-19 pandemic and successive lockdowns led to schools closing, and online education further paved the way for lesser gaps in adolescent-technology interactions. Adolescents have become more familiar with mobile phones, the internet, laptops, social media, etc. The environment in which young people are making decisions related to SRH is also rapidly evolving. Rates of sexual initiation during young adulthood are rising in many developing countries.[2] As per the National Family Health Survey (NFHS) 5 report of India, those aged 15-19 years who were already mothers or pregnant at the time of the survey was 6.8 %. The adolescent fertility rate for women aged 15-19 years was 43.8. According to the NFHS 5 report of Kerala, 2019-20, the total number of women aged 15-19 years who were already mothers or pregnant at the time of the survey was 1.8 % in urban and 3.0 % in rural areas.[9] The World Health Organization's (WHO) mission on adolescent Sexual and Reproductive health (SRH) is to contribute to a world in which its importance is understood, accepted, and supported by adolescents themselves, their families and communities, civil society bodies, leaders, and decision-makers. [10]. A potential avenue for improving SRH outcomes for young people is effective Parent-Child communication. Health approaches should maximize the interaction between adolescents and their parents, teachers, health care providers, peer educators, etc., for proper guidance.[11] However, most of today's parents were not taught about SRH by their parents or in school, leaving them unable to pass on crucial knowledge to their children. Many adolescents lack a healthy relationship with their parents or older adults, which is necessary for open discussion regarding their concerns.[2] parents are a highly influential source of knowledge, beliefs, attitudes, and values in most cultures. Parents can shape a child's perspectives, decision-making skills, and choices.[4] They lead by example, teach by instruction, inform by self-disclosure, convince by persuasion, inspire by motivation, connect with empathy, insist with supervision, provide discipline, and convince with commitment.[12] Our country had long been under the illusion of age-old traditions and reluctant to acknowledge the changing mindsets of its youth. There remains a silence between many parents and their adolescent children regarding SRH matters. Cultural taboos, stigma, shame, and lack of parents' communication skills hinder this.[13] It is common in many schools to arrange sessions on menstrual hygiene, reproductive health, etc., but most such sessions remain open only to girl students. To a large extent, the pandemic with schools closed brought down such interactive sessions too. At the same time, it taught us various lessons and gave us numerous opportunities. Digital sexuality education options and home-based classes involving parents were adopted in various parts of the world. Kerala, though one of the most literate states in India, was not open to sex education for students, apprehensive that it would promote immorality among the youth. The state is yet to implement comprehensive sex education. Parents who believe in the age-old fact that 'their children will gradually learn when the time comes' worsen this. The discomfort many parents feel about talking to their children about sexuality further impedes their ability to provide guidance. [10,13].
Many adolescents today have patchy knowledge of SRH issues which most often comes from information shared by their same-sex peers who may not be well informed. This can lead to misinformation, and myths, making them vulnerable to unprotected sex, unwanted pregnancy, STDs, unsafe abortions, etc. Adequate information from parents may improve the knowledge of these issues. India has the largest adolescent population, and Kerala dominates healthcare and literacy; it would be interesting to identify the trends regarding communication on SRH issues. Only a few studies have investigated the transmission of SRH issues between high school students and their parents and its associated factors in Kerala. This study aimed to assess adolescents' communication with their parents on SRH issues and associated factors that may help policymakers, program planners, and implementers to design appropriate interventions to address the SRH issues of adolescents.
Objectives
1. To assess the Sexual and Reproductive Health communication between adolescent high school students and their parents.
2. To determine the facilitating factors and barriers to sexual and reproductive health communication between adolescent and their parents.
Materials & Methods
Study design: Cross-sectional study
Study setting: High schools of Thrissur district.
Study period: December 2019 to May 2021
Study population: Students from 8th, 9th, and 10th grades of schools in Thrissur district. Inclusion criteria: All children of specified qualities are willing to participate, give assent, and are present during the study period. Exclusion criteria: nil.
Sample size: The sample size was calculated using the formulae Z (1-α/2)2 pq / d2 for a cross-sectional study with 80 % of the power. A study conducted by Mersha et al. in 2016 determined that shame was an important factor for poor communication between adolescents and parents on SRH matters (26.7 %).14 considering that parameter, sample Size (N) was calculated as follows: N=Z (1-α/2)2 pq / d2; p=26.7 %; q=100-p=73.3 % d= relative Precision, taken as 20 % of the prevalence; d= 5.34. Sample size (N) =3.84x26.7x73.3/ (5.34x5.34) =263 Taking a design effect of 2, N= 263x 2= 526 Taking a non- response error of 10 %, N= 580.
Sampling method: Multistage random sampling was used. In the first stage, the list of high schools in the Thrissur district was prepared, and requests for participation were sent to 100 schools randomly selected from the list. From the schools which gave permission, 3 schools were selected by convenience sampling. Due to the Covid 19 pandemic and successive lockdowns, it was possible only to collect data from 338 adolescents from 2 schools. This sample included 200 students from 1 school and 138 from the second school.
Method of data collection: After obtaining permission from the Head of the institution, one of the schools was visited, and an overview was provided regarding SRH to the students of grades 8th,9th, and 10th. The purpose of the study was explained, and following this, questionnaires were distributed, and students were asked to fill them. Due to the Covid-19 crisis, lockdown, and subsequent closure of schools, only some responses were recorded Online- Google forms were sent via email to the students after getting permission from the Head of the institution, and SRH overview through a video lecture. The questionnaire was self-administered and in the English language. The confidentiality of their responses was assured.
Study tools: A pre-tested and validated structured questionnaire prepared based on the WHO Questionnaire for the young was used to collect data. [15] Few questions were modified to account for the cultural and regional differences expected in this study. The questionnaire consisted of 3 parts- A, B, C A: Socio-demographic details of the adolescent: age, gender, religion, place of residence, grade of studying, parents' education and occupation, living arrangement at home, number of male and female family members at home, presence of elder siblings at home, etc. were elicited. B: Communication on SRH matters: The SRH matters were divided into 11 domains- (1) private parts, (2) types of touch, (3) reaction to sexual assault, (4) pubertal changes, (5) menstruation, (6) masturbation, (7) sexual contact (8) pregnancy (9) contraception (10) Sexually transmitted diseases (11) sexual abuse. The questionnaire consisted of single-answer as well as multiple-answer questions. Each domain had to queries in which the adolescents were asked to report whether their parents had communicated with them regarding these matters. Open-ended questions were asked on what they understood by the domain. For each question to which parental communication was present, a score of 1 was given. So, in total, the communication domain was scored out of 11. The scores thus obtained were interpreted as follows: 0-3: Poor communication, 4-7: Average communication, 8-11: Good communication. C: Attitude of adolescents towards communication on SRH matters. Consisted of a set of 4 questions arranged in the form of a Likert's scale - Strongly agree, agree, neither agree nor disagree, disagree, strongly disagree. The reliability of the questionnaire was assessed with a Cronbach's alpha value of 0.8- Good reliability. A pilot study was conducted to validate the questionnaire before the study period.
Data analysis: The data obtained was coded and entered in a Microsoft Excel worksheet and analyzed using the statistical software Statistical Package for Social Sciences (SPSS Version-23). The results of baseline characteristics of the study subjects were explained in terms of frequency, percentage, mean, and standard deviation. Pearson's chi-square test analyzed the association between the level of communication and factors. Fisher's Exact Test was used when the expected count was less than 5. The reliability of the study tool was assessed using Cronbach's alpha. Binary logistic regression was also performed to predict the various factors associated with communication. The significance level was estimated with 95% confidence intervals and p-value < 0.05.
Ethical consideration: Institutional Research Committee and Ethical Committee clearance were obtained before starting the study (30/IEC/19/AIMS02 dated 20-11-2019). Permission to conduct the study was obtained from the authorities of the schools. Detailed subject information was provided to the subjects to read before taking consent. Informed and written permission was obtained from each of the study participants. There were no risks involved in the study. Ethical conduct was maintained during data collection and throughout the research process. Strict confidentiality of information was retained.
Results
The socio-demographic profile of adolescents
The mean age of the study population was 14.2 ± 0.88 years. Out of the 338 adolescents, the majority, 326(96.4 %), belonged to 13- 15 years of age, as shown in (Table 1). The majority, 196 (58 %) of the study participants were females. The majority of the adolescents, 122 (36.1 %), were in 10th grade, followed by 111(32.8 %) in 9th grade and 105 (31.1 %) in 8th grade. Most of the adolescents were residents of urban areas, 303(89.6%). Only a few, 35 (10.4 %), belonged to rural areas. The distribution of students according to religion is shown in (Table 2). The living arrangements of adolescents are shown in (Table 3). A few, 9 (2.7 %), stayed with grandparents, relatives, or in hostels. (Table 4) shows the number of male and female family members in the adolescents' homes. Out of the 338 adolescents, more than half, 188 (56 %), had no elder siblings. The distribution of adolescents according to the presence of siblings at home is shown in (Figure 1). The educational status and occupation of the parents of the study participants are given in (Table 5).
Table 1:
|
Age (years) |
Frequency (%) |
|
13 |
93 (27.5) |
|
14 |
101 (29.9) |
|
15 |
132 (39.0) |
|
16 |
12 (3.6) |
|
Total |
338 (100 |
Table 2:
|
Religion |
Frequency (%) |
|
Hindu |
147 (43.5) |
|
Christian |
167 (49.4) |
|
Muslim |
20 (5.9) |
|
Atheists |
4 (1.2) |
|
Total |
338 (100) |
Table 3:
|
Living arrangement |
Frequency (%) |
|
With both parents With father only With mother only Not with parents |
288 (85.2) 16 (4.7) 25 (7.4) 9 (2.7) |
|
Total |
338 (100) |
Table 4:
|
Number of family members |
Male family members Frequency (%) |
Female family members Frequency (%) |
|
1 |
69 (20.4) |
92 (27.22) |
|
2 |
142 (42.0) |
160 (47.34) |
|
3 |
127 (37.6) |
86 (25.44) |
|
Total |
338 (100) |
338 (100) |
Table 5:
|
Educational status & Occupation |
Father Frequency (%) |
Mother Frequency (%) |
|
Educational status Professional degree Graduate Intermediate / Diploma High school |
190 (56.2) 136 (40.2) 8 (2.4) 4 (1.2) |
136 (40.2) 196 (58.0) 6 (1.8) 0 (0) |
|
Total |
338 (100) |
338 (100) |
|
Occupation Professional Semi professional Clerical/ shop owner Skilled Semi- Skilled Unskilled Unemployed |
144 (42.6) 167 (49.4) 8 (2.4) 3 (0.9) 1(0.3) 2 (0.6) 13 (3.8) |
76 (22.5) 121 (35.8) 6 (1.7) 2 (0.6) 0 (0) 1 (0.3) 132 (39.1) |
|
Total |
338 (100) |
338 (100) |
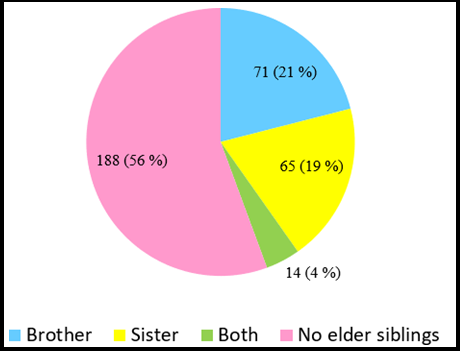
Figure 1: Distribution of adolescents according to presence of elder siblings at home (N=338)
Parent-adolescent communication on SRH matters.
The majority of the adolescents had heard about SRH matters like private parts [335(99.1 %)], Types of touch [327 (96.7 %)], Pubertal changes [329 (97.3 %)], Menstruation [318 (94.1 %)], Sexual contact [310 (91.7 %)], Pregnancy [284 (84 %)], Contraception [250 (74 %)], STDs [278 (82 %)] and Sexual abuse [307 (91 %)]. But 186 (55 %) of adolescents hadn't heard about masturbation. Adolescents' sources of information regarding SRH matters are shown in (Table 6).
Out of the 338 adolescents, parents of 255 (76.1 %) had communicated to them regarding private parts; more communication was to female adolescents [163 (63.95)]. Regarding types of touch, parents had shared; more to females than males [160 (62.2 %); 97 (37.7 %)]. Of the total, 271 (82.3 %) adolescents got parental communication regarding puberty changes, while 234 (73.5 %) were regarding menstruation. In both these SRH matters, female adolescents received a higher proportion of communication from parents [(172 (63.4 %); 185 (79.1 %)]. A lesser proportion of adolescents received parental communication regarding masturbation [27 (17.7 %); males: 16 (59.3 %); females: 11 (40.7 %)]. Only 99 (31.9 %) adolescents got a communication from parents on sexual contact; more [60 (60.6 %)] to female adolescents. A similar trend was observed regarding transmission in adolescent pregnancy [ 108 (38.0 %)]. Only very few [31 (12.4 %)] adolescents were communicated regarding contraception by parents. More communication was observed among males [16 (51.6 %)]. Regarding STDs, 66 (23.7 %) adolescents were communicated to by their parents, and 162 (52.7 %) regarding sexual abuse. In both the above said, parents had spoken more to female adolescents [35 (53 %); 105 (64.8 %)].
The distribution of communication scores of adolescents and parents based on the study tool is shown in (Figure 2). Various aspects of the discussion on SRH matters between adolescents and parents are shown in (Table 7). Out of 338 adolescents, most were comfortable discussing SRH matters with friends [221 (65.4 %)]. When it comes to parents, mothers [149 (44.1 %)] were more comfortable with SRH discussion for female adolescents [103 (69.1 %)], and fathers [50 (14.8 %)] were more comfortable for males [30 (60 %)] (Multiple answer questions). Most of the adolescents stated that their parents responded to their queries on SRH matters by giving limited information [132 (39.1 %)], unwillingly answering the question [64 (18.9 %)], or avoiding most of the questions [63 (18.6 %)]. Only 63 (18.6 %) of adolescents were answered to comfortably. 46 (13.3 %) adolescents were scolded for asking such queries. Of the 338 adolescents, 217 (64.2 %) said that their mothers were open to SRH matters discussion. 200 (59.1 %) of adolescents opined that their fathers were unavailable to discuss SRH matters. Barriers to parent- adolescent communication on SRH matters as perceived by the adolescent are shown in (Table 8). The attitude of adolescents regarding SRH communication is represented in (Table 9).
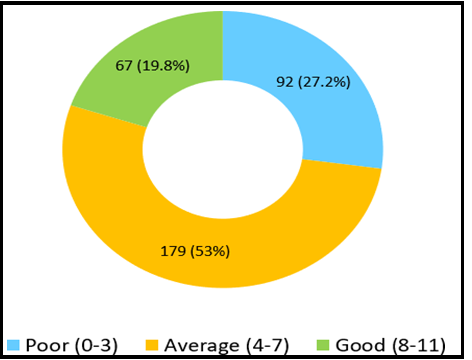
Figure 2: Distribution of Parent- Adolescent Communication Score on SRH matters
Table 6: Adolescents’ Sources of Information on SRH matters*
|
SRH matters |
Parents |
Siblings |
Media |
Teachers |
Friends |
||
|
Father |
Mother |
Brother |
Sister |
||||
|
Private parts (n= 335) |
127 (37.9) |
232 (69.3) |
17 (5.1) |
25 (7.5) |
117 (34.9) |
123 (36.7) |
63 (18.8) |
|
Types of touch (n=327) |
132 (40.3) |
231 (70.6) |
12 (3.6) |
24 (7.3) |
121 (37.0) |
136 (41.5) |
48 (14.6) |
|
Reaction to sexual assault (n=338) |
140 (41.4) |
226 (66.8) |
15 (4.4) |
25 (7.3) |
153 (45.2) |
127 (37.5) |
48 (14.2) |
|
Puberty changes (n=329) |
119 (36.2) |
190 (57.7) |
15 (4.5) |
22 (6.6) |
37 (11.2) |
190 (57.7) |
52 (15.8) |
|
Menstruation (n=318) |
84 (26.4) |
193 (60.6) |
8 (2.5) |
27 (8.4) |
43 (13.5) |
155 (48.7) |
42 (13.2) |
|
Masturbation (n=152) |
6 (3.9) |
8 (5.2) |
1 (0.6) |
2 (1.3) |
120 (78.9) |
20 (13.1) |
90 (59.2) |
|
Sexual contact (n=310) |
76 (24.5) |
105 (33.8) |
12 (3.8) |
17 (5.4) |
213 (68.7) |
85 (27.4) |
58 (18.7) |
|
Pregnancy (n=284) |
76 (26.7) |
86 (30.2) |
7 (2.4) |
5 (1.7) |
180 (63.3) |
91 (32.0) |
33 (11.6) |
|
Contraception (n=250) |
55 (22.0) |
40 (16.0) |
2 (0.8) |
1 (0.4) |
174 (69.6) |
83 (33.2) |
59 (23.6) |
|
STDs (n=278) |
64 (23) |
96 (34.5) |
0 (0) |
4 (1.4) |
208 (74.8) |
176 (63.3) |
34 (12.2) |
|
Sexual abuse (n=307) |
105 (34.2) |
134 (43.6) |
36 (11.7) |
25 (8.1) |
242 (78.8) |
70 (22.8) |
46 (14.9) |
*Each cell shows the frequency of the variable with its percentage in brackets; Multiple answers possible
Table 7:
|
7.1 Discussion on SRH matters by Adolescents(N=194) (Multiple answers) |
|||
|
With whom |
Total Frequency (%) |
Males Frequency (%) |
Females Frequency (%) |
|
Father |
65 (33.5) |
27 (41.5) |
38 (58.5) |
|
Mother |
124 (63.9) |
36 (29.0) |
88 (71.0) |
|
Others Brother Sister Teacher Doctors Friends |
11 (5.6) 33 (17.0) 16 (8.2) 42 (21.6) 113 (58.2) |
5 (45.5) 12 (36.4) 7 (43.7) 14 (33.3) 43 (38.0) |
6 (54.5) 21(63.6) 9 (56.2) 28 (66.7) 70 (62.0) |
|
7.2: Frequency of Discussion on SRH matters (N=194) |
|||
|
Frequency |
Total Frequency (%) |
Males Frequency (%) |
Females Frequency (%) |
|
Always |
6 (3.1) |
5 (83.3) |
1 (16.7) |
|
Often |
24 (12.5) |
5 (20.8) |
19 (79.2) |
|
Sometimes |
72 (37.5) |
23 (32.0) |
49 (68.0) |
|
Rarely |
92 (47.4) |
34 (37.0) |
58 (63.0) |
|
Total |
194 (100) |
67 (34.5) |
127 (65.5) |
|
7.3: Initiation of Discussion on SRH matters (N=194) |
|||
|
Initiated by |
Total Frequency (%) |
Males Frequency (%) |
Females Frequency (%) |
|
Mother |
30 (15.5) |
5 (16.7) |
25 (83.3) |
|
Father |
2 (1) |
0 (0) |
2 (100) |
|
Both parents |
32 (16.5) |
16 (50.0) |
16 (50.0) |
|
Myself |
100 (51.5) |
33 (33.0) |
67 (67.0) |
|
Depends on situation |
30 (15.4) |
13 (43.3) |
17 (56.7) |
|
Total |
194 (100) |
67 (34.5) |
127 (65.5) |
|
7.4: Reasons for Discussion with Parents (Multiple answers) (N=194) |
|||
|
Reasons |
Total Frequency (%) |
Males Frequency (%) |
Females Frequency (%) |
|
Apprehension on pubertal changes |
112 (57.7) |
28 (25.0) |
84 (75.0) |
|
Movie scene |
71 (36.6) |
32 (45.1) |
39 (54.9) |
|
Like a girl/ boy |
58 (29.9) |
22 (37.9) |
36 (62.1) |
|
Doubts regarding an advertisement |
51 (26.3) |
18 (35.3) |
33 (64.7) |
|
Others (news/ books) |
13 (6.7) |
7 (53.8) |
6 (46.2) |
Table 8: Barriers for SRH Communication by parents as perceived by adolescents*
|
SRH matters |
Culturally unacceptable (%) |
Feeling of Shame (%) |
Ignorance (%) |
Lack of communication skill (%) |
Over-confidence on adolescents’ awareness (%) |
*Others (%) |
|
Private parts |
13 |
18 |
2 |
13 |
35 |
8 |
|
(n=80) |
(16.2) |
(22.5) |
(2.5) |
(16.2) |
(43.7) |
(10.0) |
|
Types of touch |
8 |
13 |
2 |
11 |
37 |
10 |
|
(n=70) |
(11.4) |
(18.5) |
(2.8) |
(15.7) |
(52.8) |
(14.2) |
|
Puberty |
13 |
17 |
4 |
8 |
36 |
9 |
|
(n=51) |
(25.4) |
(33.3) |
(7.8) |
(15.6) |
(70.5) |
(17.6) |
|
Menstruation |
9 |
23 |
4 |
4 |
17 |
35 |
|
(n=84) |
(10.7) |
(27.3) |
(4.7) |
(4.7) |
(20.2) |
(41.6) |
|
Masturbation |
94 |
100 |
11 |
15 |
23 |
14 |
|
(n=125) |
(75.2) |
(80.0) |
(8.8) |
(12.0) |
(18.4) |
(11.2) |
|
Sexual contact |
71 |
99 |
1 |
44 |
33 |
40 |
|
(n=211) |
(33.6) |
(46.9) |
(0.4) |
(20.8) |
(15.6) |
(18.9) |
|
Pregnancy |
60 |
40 |
7 |
43 |
24 |
34 |
|
(n=176) |
(34) |
(22.7) |
(3.9) |
(24.4) |
(13.6) |
(19.3) |
|
Contraception |
74 |
42 |
25 |
73 |
33 |
57 |
|
(n=219) |
(33.7) |
(19.1) |
(11.4) |
(33.3) |
(15.1) |
(26.0) |
|
STDs |
47 |
54 |
99 |
74 |
30 |
20 |
|
(n=212) |
(22.1) |
(25.4) |
(46.6) |
(34.9) |
(14.1) |
(9.4) |
|
Sexual abuse |
48 |
63 |
2 |
62 |
26 |
27 |
|
(n=145) |
(33.1) |
(43.4) |
(1.3) |
(42.7) |
(17.9) |
(18.6) |
|
*Multiple answers were possible; *Others: ‘Parents are busy’, ‘Why should I know?’, ‘I am too young to know all that’, ‘I don’t know why’, ‘It’s a sin’ |
||||||
Table 9: Attitude of adolescents’ towards SRH Communication(N=338)
|
Statements |
Strongly disagree (%) |
Disagree (%) |
Neither agree nor disagree (%) |
Agree (%) |
Strongly agree (%) |
|
It is important to discuss sexual and reproductive health matters with parents |
12 (3.6) |
14 (4.1) |
72 (21.3) |
140 (41.4) |
100 (29.6) |
|
There is no need to discuss SRH matters with parents since all information is available from internet |
98 (29.0) |
112 (33.1) |
78 (23.1) |
36 (10.7) |
14 (4.1) |
|
There is no need to discuss SRH matters with parents since teachers will teach me better |
77 (22.8) |
98 (29.0) |
101 (29.9) |
50 (14.8) |
12 (3.5) |
|
It is uncomfortable to discuss SRH matters with parents |
35 (10.4) |
99 (29.3) |
74 (21.9) |
75 (22.2) |
55 (16.2) |
*Each cell shows the frequency of the variable with its percentage in brackets
Association between socio-demographic characteristics of adolescents and SRH communication
Out of 338 adolescents, 45 (34.1 %) 15-year-olds had poor communication, followed by 26 (25.74 %) 14-year-olds, while good communication was maximum among 16-year-old [3 (25.1 %)] followed by 14-year-olds [24 (23.6 %)]. The group differences were not statistically significant (p =0.209). Of 338 adolescents, 58 (40.8%) male adolescents had poor communication, while only 24 (17 %) had good communication. Among the female adolescents, 43 (22 %) had good communication, and only 34 (17.3 %) had poor SRH communication. The difference between the groups was statistically significant (p = 0.001). Of the 338 adolescents, 44 (36.1 %) in the 10th grade had poor communication, and only 18 (14.7 %) had good communication. The proportion of poor communication was 23 (22 %) among 8th grade and 25 (22.5 %) among 9th-grade adolescents. The difference between the groups was insignificant (p =0.072). Out of the 338 adolescents, 81 (26.7 %) urban area residents had poor SRH communication, while 59 (19.5 %) had good communication. There was no association between adolescents' place of residence and SRH communication (p=0.66). Out of the total adolescents, 37 (25.2 %) Hindus, 45 (27 %) Christians, 8 (40 %) Muslims, and 2 (50 %) atheists had poor SRH communication. Good SRH communication was seen only in 28 (19 %) Hindus, 35 (20.9 %) Christians, 3 (15 %) Muslims, and 1 (25 %) atheists. There was no association between adolescents' religion and SRH communication. Of the 338 adolescents, 288 (85.3 %) stayed with both parents (p =0.733). Among them, 80 (27.8 %) had poor communication, while only 56 (19.4 %) had good communication. Among those who stayed with their mother only, an equal number [3 (18.7 %)] had poor and good SRH communication. 7 (28 %) of those staying with fathers only had good communication. A few adolescents did not stay with their parents [9 (2.7 %)]. Of them, 4(55.6 %) had poor SRH communication, while only 1(11.1%) had good communication. There was no association between adolescents' living arrangements at home and SRH communication (p=0.407). Out of the 338 adolescents, poor SRH Communication was found among 17 (18.5 %) of those with 1 male family member, 42 (26.25 %) of those with 2 males at home and 33 (38.4%) of those with 3 males at home. Of those who had 1 male at home, 22 (23.9 %) had good SRH communication, while 29 (18.12 %) among those with 2 male members at home and 16 (18.6 %) of those with 3 males at home had good SRH communication. The difference between the groups was statistically significant (p = 0.043). Of the 338 adolescents, 150 (44.3 %) had elder siblings. Among them, 71 (21 %) had brothers only as siblings. Of these, 22 (31 %) adolescents with only brothers as elder siblings had poor SRH communication, while only 15 (21.1 %) had good communication. Out of the adolescents with only sisters as elder siblings, 17 (26.1 %) had poor communication, while 11 (16.9 %) had good communication. Of adolescents with brothers and sisters as elder siblings, 4 (28.6 %) had poor SRH communication, while only 1 (7.2 %) had good communication. Of the 188 (55.7 %) adolescents with no elder siblings, 49 (26.1 %) had poor SRH communication. The differences observed between the groups were not statistically significant (p =0.757). There was no association between the presence of elder siblings at adolescents' homes and SRH communication. Of the adolescents whose fathers were in professional occupations, 38 (26.4 %) had poor SRH Communication, while only 28 (19.4 %) had good communication. When it comes to semi-professional jobs also, good communication [34(20.4 %)] is less compared to poor [49 (29.3 %)]. In the case of unemployed father, good communication was better [3 (23.2 %)] compared to poor [2 (15.3 %)]. The group differences were not statistically significant (p =0.703). There was no association between adolescents' father's occupation status and SRH communication. Among mothers who were professional degree holders, 37 (27.2 %) had poor SRH communication, and only 33 (24.3 %) had good communication. When the mother was a graduate, there was poor communication in 54 (27.6 %), while good communication was only in 32 (16.3 %). But, when the mother's education level was intermediate/ diploma, good communication was in 2 (33.3 %) and poor SRH communication in 1 (16.7 %). The difference between the groups was insignificant (p =0.381). There was no association between adolescents' mothers' education status and SRH communication. The association between the attitude of adolescents and SRH communication is represented in (Table 11).
Binary logistic regression was used to find out the facilitating factors of SRH Communication. The variables with a p-value less than 0.05 in the bivariate analysis were included in the regression model, including gender, number of females at home, and number of males at home. As shown in (Table 12), in the regression analysis, female adolescents had more SRH communication than males, with an odds ratio (OR) of 1.206 (0.65-2.21). More number of females was a factor for good SRH communication with an odds of 1.23 (0.83-1.81). Lesser number of males at home was a factor for good communication, with an odd's ratio of 0.91(0.61-1.35). The Odds ratio was not statistically significant.
Table 10: Association between Socio-demographic characteristics and SRH Communication
|
Age |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.209 |
||
|
13 |
19 (20.4) |
53 (57) |
21 (22.6) |
93 (100) |
|
|
14 |
26 (25.74) |
51 (50.5) |
24 (23.76) |
101 (100) |
|
|
15 |
45 (34.1) |
68 (51.5) |
19 (14.4) |
132 (100) |
|
|
16 |
2 (16.6) |
7 (58.3) |
3 (25.1) |
12 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
|
Fisher’s exact value=8.413; df=6 |
|||||
|
Gender |
SRH Communication |
Total (%) |
*p value Chi square test |
||
|
Poor (%) |
Average (%) |
Good (%) |
|||
|
Male |
58 (40.8) |
60 (42.2) |
24 (17.0) |
142 (100) |
0.001 |
|
Female |
34 (17.3) |
119 (60.7) |
43 (22.0) |
196 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
*Chi square value=22.948; df=2
|
Grade |
SRH Communication |
Total (%) |
p value Chi square test |
||
|
Poor (%) |
Average (%) |
Good (%) |
|||
|
8th |
23 (22.0) |
59 (56.1) |
23 (21.9) |
105 (100) |
0.072 |
|
9th |
25 (22.5) |
60 (54.1) |
26 (23.4) |
111 (100) |
|
|
10th |
44 (36.1) |
60 (49.2) |
18 (14.7) |
122 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Chi square test value=8.595; df=4
|
Religion |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.733 |
||
|
Hindu |
37 (25.2) |
82 (55.8) |
28 (19) |
147 (100) |
|
|
Christian |
45 (27.0) |
87 (52.1) |
35 (20.9) |
167 (100) |
|
|
Muslim |
8 (40.0) |
9 (45.0) |
3 (15.0) |
20 (100) |
|
|
Atheist |
2 (50.0) |
1 (25.0) |
1 (25.0) |
4 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value= 3.581; df=6
|
Living Arrangement |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.407 |
||
|
With both parents |
80 (27.8) |
152 (52.8) |
56 (19.4) |
288 (100) |
|
|
With mother only |
3 (18.75) |
10 (62.5) |
3 (18.75) |
16 (100) |
|
|
With father only |
4 (16.0) |
14 (56.0) |
7(28.0) |
25 (100) |
|
|
Not with parents |
5 (55.6) |
3 (33.3) |
1 (11.1) |
9 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value=6.146; df=6
|
Number of females at home |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.001 |
||
|
1 |
35 (50.7) |
24 (34.8) |
10 (14.5) |
69 (100) |
|
|
2 |
32 (22.54) |
82 (57.75) |
28 (19.71) |
142 (100) |
|
|
3 |
25 (19.7) |
73 (57.5) |
29 (22.8) |
127 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
*Chi square value=24.779; df=4
|
Number of males at home |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.043 |
||
|
1 |
17 (18.5) |
53 (57.6) |
22 (23.9) |
92 (100) |
|
|
2 |
42 (26.25) |
89 (55.63) |
29 (18.12) |
160 (100) |
|
|
3 |
33 (38.4) |
37 (43.0) |
16 (18.6) |
86 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
*Chi square value= 9.835; df=4
|
Elder siblings at home |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.757 |
||
|
Brother |
22 (31.0) |
34 (47.9) |
15 (21.1) |
71 (100) |
|
|
Sister |
17 (26.1) |
37 (57.0) |
11 (16.9) |
65 (100) |
|
|
Both |
4 (28.6) |
9 (64.2) |
1 (7.2) |
14 (100) |
|
|
No elder siblings |
49 (26.1) |
99 (52.6) |
40 (21.2) |
188 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value= 3.404; df=6
|
Father’s educational status |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.494 |
||
|
Professional degree |
48 (25.3) |
102 (53.6) |
40 (21.1) |
190 (100) |
|
|
Graduate |
43 (31.62) |
69 (50.73) |
24 (17.65) |
136 (100) |
|
|
Intermediate/ diploma |
1 (12.5) |
5 (62.5) |
2 (25.0) |
8 (100) |
|
|
High school |
0 (0) |
3 (75.0) |
1 (25.0) |
4 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value=5.4; df=6
|
Father’s occupational status |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.703 |
||
|
Professional |
38 (26.4) |
78 (54.2) |
28 (19.4) |
144 (100) |
|
|
Semi professional |
49 (29.3) |
84 (50.3) |
34 (20.4) |
167 (100) |
|
|
Clerical/ shop owner |
1 (12.5) |
6 (75.0) |
1 (12.5) |
8 (100) |
|
|
Skilled |
1 (33.3) |
2 (66.7) |
0 (0) |
3 (100) |
|
|
Semi- skilled |
1 (100.0) |
0 (0) |
0 (0) |
1 (100) |
|
|
Unskilled |
0 (0) |
1 (50.0) |
1 (50.0) |
2 (100) |
|
|
Unemployed |
2 (15.3) |
8 (61.5) |
3 (23.2) |
13 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value=9.001; df=12
|
Mother’s educational status |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.381 |
||
|
Professional degree |
37 (27.2) |
66 (48.5) |
33 (24.3) |
136 (100) |
|
|
Graduate |
54 (27.6) |
110 (56.1) |
32 (16.3) |
196 (100) |
|
|
Intermediate/ diploma |
1 (16.7) |
3 (50.0) |
2 (33.3) |
6 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Fisher’s exact value=4.192; df=4
|
Mother’s occupational status |
SRH Communication |
Total (%) |
p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.096 |
||
|
Professional |
15 (19.7) |
38 (50.0) |
23 (30.3) |
76 (100) |
|
|
Semi professional |
31 (25.6) |
67 (55.3) |
23 (19.1) |
121 (100) |
|
|
Clerical/ shop owner |
1 (16.6) |
5 (83.4) |
0 (0) |
6 (100) |
|
|
Skilled |
0 (0) |
1 (50.0) |
1 (50.0) |
2 (100) |
|
|
Unskilled |
0 (0) |
1 (100.0) |
0 (0) |
1 (100) |
|
|
Unemployed |
45 (34.0) |
67 (51.0) |
20 (15.0) |
132 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
Table 11: Association between attitude of adolescents and SRH communication
|
Attitude 1: It is important to discuss sexual and reproductive health issues with parents |
|||||
|
Attitude |
Communication |
Total (%) |
*p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
0.001 |
||
|
Strongly disagree |
4 (33.33) |
4 (33.33) |
4 (33.33) |
12 (100) |
|
|
Disagree |
6 (42.9) |
7 (50.0) |
1 (7.1) |
14 (100) |
|
|
Neither agree nor disagree |
26 (36.1) |
43 (59.7) |
3 (4.2) |
72 (100) |
|
|
Agree |
39 (27.9) |
73 (52.1) |
28 (20.0) |
140 (100) |
|
|
Strongly agree |
17 (17.0) |
52 (52.0) |
31 (31.0) |
100 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
|
*Fisher’s exact value=30.21; df=8 |
|||||
|
|
|||||
|
Attitude 2: There is no need to discuss SRH matters with parents since all information is available from internet |
|||||
|
Attitude |
Communication |
Total (%) |
*p value Fisher’s exact test |
||
|
Poor (%) |
Average (%) |
Good (%) |
|||
|
Strongly disagree |
16 (16.32) |
56 (57.14) |
26 (26.53) |
98 (100) |
0.001 |
|
Disagree |
24 (21.4) |
60 (53.6) |
28 (25.0) |
112 (100) |
|
|
Neither agree nor disagree |
31 (40.0) |
37 (47.0) |
10 (13.0) |
78 (100) |
|
|
Agree |
11 (30.5) |
23 (63.9) |
2 (5.6) |
36 (100) |
|
|
Strongly agree |
10 (71.43) |
3 (21.43) |
1 (7.14) |
14 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
|
*Fisher’s exact value=34.73; df=8 |
|||||
|
Attitude 3: There is no need to discuss SRH matters with parents since teachers will teach me better |
|||||
|
Attitude |
Communication |
Total (%) |
p value Fisher’s exact test
|
||
|
Poor (%) |
Average (%) |
Good (%) |
|||
|
Strongly disagree |
21 (27.2) |
36 (46.8) |
20 (26) |
77 (100) |
0.368 |
|
Disagree |
22 (22.45) |
54 (55.1) |
22 (22.45) |
98 (100) |
|
|
Neither agree nor disagree |
29 (28.7) |
55 (54.5) |
17 (16.8) |
101 (100) |
|
|
Agree |
18 (36.0) |
25 (50.0) |
7 (14.0) |
50 (100) |
|
|
Strongly agree |
2 (16.7) |
9 (75.0) |
1 (8.3) |
12 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
|
Fisher’s exact value=8.699; df=8 |
|||||
|
Attitude 4: It is uncomfortable to discuss SRH matters with parents |
|||||
|
Attitude
|
Communication |
Total (%) |
*p value Chi square test
|
||
|
Poor (%) |
Average (%) |
Good (%) |
|||
|
Strongly disagree |
4 (11.4) |
17 (48.6) |
14 (40) |
35 (100) |
0.001 |
|
Disagree |
16 (16.2) |
50 (50.5) |
33 (33.3) |
99 (100) |
|
|
Neither agree nor disagree |
20 (27.0) |
41 (55.4) |
13 (17.6) |
74 (100) |
|
|
Agree |
30 (40.0) |
39 (52.0) |
6 (8.0) |
75 (100) |
|
|
Strongly agree |
22 (40.0) |
32 (58.2) |
1 (1.8) |
55 (100) |
|
|
Total |
92 (27.2) |
179 (53.0) |
67 (19.8) |
338 (100) |
|
|
*Chi Square value=46.85; df=8 |
|||||
Table 12: Regression Analysis on the facilitating factors and SRH Communication
|
Variables |
B |
S.E. |
Wald |
df |
p |
OR |
95% C.I. for OR |
|
|
Lower |
Upper |
|||||||
|
Gender |
0.187 |
0.310 |
0.364 |
1 |
0.546 |
1.206 |
0.657 |
2.215 |
|
Number of females |
0.207 |
0.199 |
1.087 |
1 |
0.297 |
1.230 |
0.833 |
1.816 |
|
Number of males |
-0.088 |
0.201 |
0.193 |
1 |
0.660 |
0.915 |
0.617 |
1.358 |
Discussion
Parent-Adolescent Communication on Sexual and Reproductive Health (SRH) matters.
The present study found that the majority of the adolescents [179 (53 %)] had average communication (discussed 4-7 SRH matters) on SRH matters. This was followed by poor communication (discussed 0- 3 SRH matters) [92(27.2 %)] and good communication (discussed 8-11 SRH matters) only in 67 (19.8 %). This was consistent with a study among high school students in Eastern Ethiopia, where only 37 % of students discussed at most minuscule 2 SRH topics with their parents.[16] A study by Mersha et al. also showed similar results.[14] Another study from the Wollega zone reported that 32.5 % of females and 32.7 % of males discussed SRH matters with parents.[17] In the present study, 57.4 % of adolescents discussed with parents (males: 35.3 %; females: 64.7 %). A different finding was obtained from Debre Markos town, where 68.2 % of adolescents had communicated with other family members on SRH matters.[18] The situation in India was different. Both mothers and fathers reported limited communication on SRH matters. Communication was somewhat better when the sex of the parent and adolescent were the same. The parent–adolescent sexual contact was infrequent, fear-based, unidirectional, and does not encourage questions, and is of poor quality, as identified by Byers et al. [19] In the present study, SRH communication favored females in every matter. Only in the case of masturbation do males have better communication with their parents. While in Kenya, according to Beatrice et al., more girls than boys reported that their parents had talked to them about sexual relationships, and more parents reported having had conversations about sexual relationships with their daughters compared to sons. This tilt in favor of girls in parent-child communication was driven by the perception that girls' vulnerability to sexual risks was much higher than boys. [20]
In this study, 63.9 % of adolescents discussed SRH matters with mothers, females more than males, and only 33.5 % with fathers. A similar finding was observed in a study conducted by Agrawal et al.; in most instances, only mothers were involved in discussions about reproductive health problems, while fathers' involvement was zero percent.[21] Also, in a study conducted at Mysore City by Ahmed et al., 95 % of the study subjects had never discussed sexual health-related matters with fathers, and 85.32 % of them with mothers there. [22] But, in an Ethiopian study, communication was only 14.7 % with mothers and 3.9 % with fathers.[18] The present study showed that following parents, adolescents preferred their friends to discuss SRH matters. But, in a study by Abebe et al., the communication on SRH matters was 9 % with boys or girlfriends, 23.4 % with same-sex peers, and 5.7 % with the opposite sex.[18] In the present study, 5.6 % and 17 % of adolescents discussed SRH matters with brothers and sisters, respectively. But the discussion of SRH matters with siblings from another study was 15 %, and it was 2.1 % with other family members.[18] Three fourth of students preferred their peers to discuss their SRH matters. However, students also discussed these with mothers, sisters, brothers, and fathers. Students discussed 2.9 times more with their mothers and 2.8 times more with their brothers and sisters, respectively, about SRH than other family members. 16 This study had 8.2 % of adolescents discussing with teachers and 21.6 % with health personnel, 5 % with health personnel, and 11.1 % with teachers in a study in Ethiopia. [18] In this study, female adolescents have discussed SRH matters more with mothers and fathers than male adolescents. But according to Dessalegn et al., in Ethiopia, female, young people reported having discussed with their mothers and sisters while young male people reported having discussed with their fathers and brothers; more communication takes place between mothers and daughters (20.9 %) compared to fathers and sons (5.7 %). [17] Participants' brothers were the most preferred family members (11.2 %) to communicate with about SRH matters, followed by fathers, who accounted for 10.2 %. [23] About 21.3 % of students in a Vienna study had discussed at least four topics of SRH with their parents; male adolescents discussed the topics more frequently with their parents than female adolescents (29.2 % versus 16.1 %). Moreover, male participants discussed SRH matters with their fathers and mothers more often than female participants. These results highlight that boys talk more than girls to their parents about SRH. However, more adolescent boys and girls talk with their mothers than their fathers. [24] According to Soltani et al., only 29 % of adolescents had talked to their male parent on SRH subjects, of which 63 % had rarely discussed the matter. Over 50 % of the subjects had spoken to their mother, of which 39% had done this rarely.41.3 % of the adolescents reported talking with their older siblings, of which 49.6 % had done this only occasionally.[25] In the present study, parents of 76.1 % had communicated regarding private parts; more communication was to female adolescents. Regarding types of touch, parents of 78.5 % of adolescents had communicated: more to females than males. Regarding responses against sexual assault, only 68.9 % of adolescents had communication from their parents. Females got more communication from parents in this matter. Of the total, 82.3 % of adolescents got parental communication regarding puberty changes, while 73.5 % were regarding menstruation. In both these SRH matters, female adolescents received more communication from parents. But a lesser proportion of adolescents received parental communication regarding masturbation [27 (17.7 %); males: 16 (59.3 %); females: 11 (40.7 %)]. Regarding sexual contact, only 31.9 % of adolescents got a communication from parents: more female adolescents. A similar trend was observed regarding communication on adolescent pregnancy. Only very few adolescents were communicated regarding contraception by parents. More communication was observed among males in this matter. In the context of STDs and sexual abuse, less than a quarter of adolescents were communicated to by their parents. In both of the above said parents communicated more with female adolescents. But, according to a study by Dessalegen et al., only a low proportion of both males (15 %) and females (10.4 %) reported having discussed with their parent's biological aspects of SRH, such as body change during puberty (20.1 % of males and 14.8% of females) while 5.7 % of males and 10.4% of females reported discussing menstruation; less than 50 % of males and females reported to discuss on preventive aspects like contraceptive methods and family planning; but about two-thirds of males and females, reported to have discussed on associated risk aspects of SRH like unwanted pregnancy and HIV/AIDS.17 In another study, the respondents who had discussed STI/HIV/AIDS was 34.6 %. Among those students,25.7 % discussed with their friends, followed by their mother; 28.5 % reported discussing unwanted pregnancy. Among those respondents, 20.5 % had discussed unwanted pregnancy with their friends, and 20.3 % with their mother. 27.6 % of the respondents discussed premarital sex, and 21.1 % and 15.3 % had discussed it with friend/s and mothers, respectively. About 72.4 % of the respondents didn't discuss premarital sex.[26] In Dire Dawa, parents reported discussing human growth and development, pregnancy, childbirth, and abortion; half had discussed STIs; contraception was the least discussed; only 16 % of parents had discussed all SRH topics in Dir e Dawa. 16 Yadeta et al. reported that HIV/AIDS was the more frequent topic of communication with mothers (51.92 %) and fathers (38.74 %). Reproductive organ growth and development was second, communicated by 26.68 % of mothers and 14.77 % of fathers. The condom was the least communicated topic. More communication was made with the mothers compared to the father.[27] As per the results of this study, out of 194 adolescents who discussed SRH matters with parents, 47.4% did it rarely, 37.5% discussed it sometimes, and 12.5 % often. According to Soltani et al., only 29 % of adolescents had talked to their male parents on SRH subjects, of which 63 % had rarely discussed the matter. Over 50 % of the subjects had spoken to their mother, of which 39% had done this rarely. 41.3% of the adolescents reported talking with their older siblings, of which 49.6 % had done this only occasionally. [25] In most instances, according to the present study, the adolescent initiated the discussion (51.5 %). This was followed by parents (16.5 %) initiating the discussion on SRH matters. But the Parent-young people communication on SRH was usually initiated by parents according to research by Dessalegn et al. [17] Mothers were the most frequent initiators of discussions in Dire Dawa.16 The most common reason the discussion happened was apprehension regarding puberty changes in the body, according to the present study (57.7 %), more for females than males (75 % versus 25 %). This was followed by discussions initiated following co-watching movies and doubts that arose after a movie scene or advertisement (36.6 %). But in a study in Kenya, the most common trigger for SRH discussion was romantic relationships of adolescents (55.4 %), followed by the wearing of non-traditional clothing by girls (40.1 %).
[20] In this study, the female adolescents were more comfortable discussing SRH matters with mothers, while male adolescents were comfortable with fathers. This may be because mothers were perceived to be better listeners than fathers. Fathers may find it harder to discuss potentially embarrassing relational topics and have an open conversation about sexual health with their adolescent children and may need further support in initiating such conversations. Of the 338 adolescents in this study, 64.2 % said that their mothers were open to SRH matters discussion; 59.1 % of adolescents opined that their fathers were not open to discussion on SRH matters. In a study by Ayalew et al., only 17.9 % of fathers and 25.4 % of mothers were transparent and willing to discuss SRH matters.16 Regarding the preferred group for discussion about SRH matters, most (76.4 %) choose their friends, followed by brothers (27 %), teachers (24.1 %), mothers (23.8 %), fathers (20.7 %), and sisters (20.4 %).26 Moreover, there were sex preferences in discussing SRH matters in this study and others. Both males and females were more comfortable discussing SRH with gender matching. Most adolescents in the present study stated that their parents responded to their queries on SRH matters by giving limited information, unwillingly answering, or avoiding most questions. Outcomes of a study in Kenya point to four communication approaches: no communication; fear-based communication; supportive communication; communication involving an external person. In the first, parents perceived adolescents as too young for SRH communication, and the other three approaches focused on delaying the age when adolescents began engaging in romantic relations.[20]
Factors affecting Parent-adolescent SRH communication.
Association between Sociodemographic Characteristics of Adolescents and SRH Communication
In the present study, the mean age of the study population was 14.2 ± 0.88 years. 96.4 % belonged to 13- 15 years of age. In the Hadiya zone study, the participants were 15 to 19 years old, with a mean age of 17.73 + 1.18 SD years. [23] In the current study, 34.1 % 15-year- olds had poor communication, followed by 25.74 % 14-year-olds. This study had no association between the age of adolescents and SRH communication. In a study conducted in Ethiopia, among younger people (10–14 years), only one-fifth of males and one–third of females reported parental communication. Males were less likely to discuss at an early age than females of the same age group. This proportion increased to one-third for both females and males at ages 15–19 years and declined at the age 20–24 years. Relatively more communication seemed to occur at 15-16 years for females and at 17– 18 years for males. [26] Majority of the study participants were females in this study. 40.8 % of male adolescents had poor communication, and only 17 % had good communication. Among the female adolescents, 22 % had good communication, and 17.3 % had poor SRH communication. Female gender was identified as a facilitating factor for SRH communication. On regression analysis, the female gender had more SRH communication than males, with an odds ratio of 1.206 (0.652.21). Similar results were observed in Boditi town (OR:1.4) and Eastern Ethiopia, where the odds of discussing SRH issues were 40 % less in males compared to female students.
[16] The sexual vulnerability the group faces in society may be the reason behind this finding. While in West Ethiopia, studies did not show any association between gender. [26] There was no association between adolescents' grades studying and SRH communication in this study. But in Northwest Ethiopia, grade 12 students were less likely to communicate on SRH issues than grade 9 students (Adjusted OR = 0.4; 95 % CI 0.2 to 0.7). [26] Lower grade (grade 9) participants were about 3 times more likely to communicate about SRH matters than higher grades participants (grade twelve and above), according to Samuel et al. [23] In the present study, there was no association between adolescents' place of residence and SRH communication. Similar findings were observed in other countries as well. This study had no association between adolescents' religion and SRH communication; 40 % of Muslims had poor SRH communication. In the study by Dessalegn et al., those who reported attending religious ceremonies more frequently were more likely (59.4 %) to report parent communication than those who reported infrequent attendance (35.7 %). [17] Those who were in grades 9 and 10 were two times more likely to communicate compared to those in grades 11 and 12, those who attended churches/mosques were five times more likely to have communication with their parents on SRH issues, and students whose previous residence was at urban were 2.26 times more likely to have parent-adolescent communication according to findings by Abebe et al.[18] Young people living in urban were more likely to report sexuality communication with parents than semi-urban dwellers (AOR = 2.81; 95 %CI = 1.83-4.31) in West Ethiopia.[17] In the present study 85.3 % adolescents stayed with both parents. There was no association between adolescents' living arrangements at home and SRH communication. According to an Ethiopian study, about one-third of males and females living with both parents reported discussing SRH topics with parents there. Relatively a higher proportion of males living with their fathers and females living with other relatives reported discussing more SRH health topics than those young people living in other living arrangements. [17] In the present study, the SRH communication was good when 3 female family members were at the adolescents' home compared to 1 or 2 females. The difference observed was statistically significant. More females at home facilitate SRH communication [OR: 1.23 (0.83 analysis, it was found to be 1.81)]. But on regression not significant. Also, when the number of males was less, the SRH communication was good. Lesser number of males at home was a facilitating factor for good communication [OR: 0.91(0.61-1.35)]. But on regression analysis, it was found to be not significant. But those students whose family size was less than three were less likely to communicate compared to those whose family size was greater than seven (Adjusted OR = 0.5; 95 % CI 0.2 to 0.9) in a study in Northwest Ethiopia. 26 This may be because females considered themselves at high risk for sexual exploitations. In the present study, there was no association between the presence of elder siblings at adolescents' homes and SRH communication. While in Johannesburg, the presence of young er siblings were identified as a barrier to not discussing sexual matters openly within the family. Parents felt that conversations about sexual matters were restricted because the content would be inappropriate for younger siblings. [28] There was no association between adolescents' parents' education status and SRH communication, according to this study. This was consistent with findings of a Vietnam study by Visani et al. [24] Parent-adolescent communication was significantly associated with paternal educational status as per a study by Abebe et al. Fathers with educational status of college and above were 2 times more likely to have communication on SRH matters compared to illiterates. From the maternal educational status, those from grades 7-12 were 3 times more likely to have communication with their adolescents (95 % CI=2.69 (1.26- 5.73). 18 Students whose mother was able to read and write were 2 times more likely to communicate SRH issues with their parents than those students whose mother were unable (Adjusted OR = 2) according to Shiferaw et al. [26] As per this study, there was no association between adolescents' parents' occupation status and SRH communication. Similar results were obtained by research by Visany et al. Most mothers were housewives in both situations. [24] But according to Nurilign et al., civil servant fathers were 5.34 times more likely to communicate (95 % CI=5.34(1.72-16.58), but other categories of occupational status were not associated with SRH communication.[18]
Association between the attitude of adolescents and SRH communication
In this study, most adolescents had a solid positive attitude towards SRH communication, and they had a good level of communication. Those who had a strong negative attitude toward SRH communication had poor communication. But, in an Ethiopian study, more than two third (69.5 %) of the young people perceived that discussing SRH matters with parents was difficult.[17] About 70.8 % of males and females had positive attitudes towards and accepted the importance of discussing SRH matters with their parents in the study by Visany et al. [24] Adolescents' perceived importance of discussing SRH issues with parents was a facilitating factor for SRH communication. On the other hand, the negative attitudes of adolescents were a barrier.
Barriers to SRH communication as perceived by the adolescents.
According to the present study, the parents' overconfidence in the adolescent's awareness of SRH matters was the most common barrier to communication between parents and adolescents in private parts, types of touch, and puberty. Regarding menstruation, the primary barrier, as perceived by the adolescents, was busy parents; they were too young to know all that, etc. Cultural barriers and feelings of shame were the primary reasons for the noncommunication on masturbation by parents. Shame was the primary barrier to communication in the context of sexual contact, and 34 % of adolescents perceived that their parents did not communicate with them during pregnancy as it was culturally unacceptable. Cultural unacceptability and lack of communication skills in parents were significant barriers to SRH communication on contraception. Ignorance of parents was an important barrier to communication regarding STDs. The barriers to SRH communication on sexual abuse were feeling of shame and parents' lack of communication skills. The fear of parents, an embarrassment in discussing with parents, the taboo attached to sex and parents' failure to give time to listen, and parents' lack of interest in discussing were the barriers to SRH communication identified by Dessalegn et al. [17] The lack of perceived parental knowledge, intergenerational cultural taboos made parent young people communication challenging. Culture, shame, and lack of knowledge were identified as significant communication barriers in Boditi town.
[29] As per Kegaugetse's study, adolescents revealed that they do not openly communicate with their parents because their parents were strict, and they feared that they would be embarrassed and misunderstood. Cultural beliefs acted as an inhibiter in addressing issues of sex. Also, religious beliefs guide parents on what to discuss with their children. They focused on teaching their daughters about the virtues of virginity and that they should forget about sexual activities until they got married. This barrier hindered them from talking with their children about SRH. [30] Cultural taboos, shame, lack of communication skills in parents, etc., were reasons that withheld communication in Dire Dawa.[16] According to Shiferaw et al., the majority of the respondents did not discuss STI/HIV/AIDS because of parents' lack of knowledge, followed by parents' lack of communication skills; 22.7 % didn't know the reasons why they didn't discuss unwanted pregnancy with their parents.[26] Those adolescents who had no information about the availability of adolescent-friendly health facilities were less likely to communicate with their parents about SRH, as identified by Samuel et al. [23] Adolescents who were more likely to practice poor/abysmal SRH communication were those who had poor behavioral beliefs on communicating sexual issues with parents and those who perceived their parents' reproductive health (RH) knowledge as poor, according to Yadeta et al.[27] In a research done in 2013 in Kerala, regarding pregnancy among unmarried adolescents and young adults, found a strong association between unmarried adolescent pregnancy and lack of parental supervision and control, poor intrafamily relationship, family problem, lack of knowledge on SRH.[28]
Conclusion
The present study was done to assess the SRH communication between adolescent high school students and their parents in the Thrissur district and to determine its facilitating factors and barriers. Media was the most common source of information regarding SRH.
The scope of topics of parent-adolescent communication on SRH was primarily limited to issues related to pubertal development and protection from sexual harassment and abuse. Most had average SRH communication, followed by poor communication; very few adolescents had good SRH communication. Gender matching was observed regarding SRH communication. The frequency of discussion was rare. The adolescent themselves initiated the debate; it was in sporadic instances that parents started it. Most parents gave limited information, unwillingly answered the question, or avoided most questions. The majority said that their mothers were open to SRH matters discussion, while fathers were not. Bivariate analysis showed a statistically significant association between SRH communication and adolescents' gender, number of males and females at home, and positive attitude towards SRH communication (p < 0.05). More number of females and a lesser number of males at home was a factor for good SRH communication. Contact was found to be more to 1.2 times more for female adolescents. The strong positive attitude of adolescents resulted in good SRH communication. The feeling of shame, cultural unacceptability, and lack of communication skills in parents were perceived as significant barriers to communication.
Recommendations
Adolescent- Parent co-education sessions should be conducted regularly at schools or Health care facilities on SRH matters that help to reduce the perceived barriers and hesitancy for communication. Interactive platforms may be organized at schools or healthcare facilities for parents to improve their communication skills. Parents should focus on communicating with male and female adolescents equally. Age-appropriate comprehensive sexuality education may be incorporated into their curriculum effectively to strengthen their SRH. Further research to understand the parents' perspectives on SRH communication is recommended.
Limitations
Due to the COVID-19 pandemic, a calculated sample size could not be achieved for more accurate results. Few of the responses were obtained through online Google forms. It took much work for students to express their views on the open-ended questions fully. The study could incorporate only the adolescents' perspectives on SRH communication. The study population was 13-16 years old. The adolescent age group is a broader age group from 10-19 years. The study tool being a self-administered questionnaire, the younger age groups could not be included as they needed help comprehending and answering the questions asked. Thus, the study's results cannot be generalized to all adolescent populations.
References
- World Health Organisation (WHO) Coming of age: adolescent health.
- World Health Organisation (WHO) Strengthening the health sector response to adolescent health and development.
- Hindin MJ, Fatusi AO (2009) Adolescent sexual and reproductive health in developing countries: an overview of trends and interventions. Int Perspect Sex Reprod Health. 35(2): 58-62.
- Population Reference Bureau. 2017 World Population Data Sheet with Focus on Youth.
- Ahlberg BM, Jylkäs E, Krantz I (2001) Gendered construction of sexual risks: implications for safer sex among young people in Kenya and Sweden. Reprod Health Matters. 9(17): 26-36.
- Mturi AJ (2003) Parents' attitudes to adolescent sexual behaviour in Lesotho. Afr J Reprod Health. 7(2): 25-33.
- United Nations Children's Fund (UNICEF). Sexual violence against children.
- Ministry of Health and Family Welfare of India (MOHFWI). National Family Health Survey (NFHS-5). [Online]. Available from: http://rchiips.org/nfhs/nfhs5Reports/India.pdf [Accessed 25 November 2021].
- Ministry of Health and Family Welfare of India (MOHFWI). National Family 201920 Health Survey (NFHS-5).
- Chandra-Mouli V, Bloem P, Ferguson J (2013) The World Health Organization's work on adolescent sexual and reproductive health. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 56(2): 256-61.
- Park K (2021) Parks textbook of preventive and social medicine. (26th ed.). Jabalpur, India: Bhanot Publishers.
- Pickhardt CE (2010) Psychology today. Adolescence and the Influence of Parents. Weblog.
- United Nations Programme on HIV and AIDS (UNAIDS). Global HIV & AIDS statistics — Fact sheet.
- Kinfe M, Getachew G (2018) Assessment of Communication on Sexual and Reproductive Health Issues among Gorro Preparatory School Students with their Parents Gurage Zone, Southern Ethiopia, Ethiopia. EC Gynaecology. 7(3): 95-103.
- World Health Organization (WHO). Illustrative Questionnaire for Interview- Surveys with Young People.
- Ayalew M, Mengistie B, Semahegn A (2014) Adolescent-parent communication on sexual and reproductive health issues among high school students in Dire Dawa, Eastern Ethiopia: a cross sectional study. Reprod Health. 11(1): 77.
- Tesso DW, Fantahun MA, Enquselassie F (2012) Parent-young people communication about sexual and reproductive health in E/Wollega zone, West Ethiopia: Implications for interventions. Reproductive health. 9: 13.
- Abebe N, Mullu N (2013) Assessment of Parent Adolescent Communication on Sexual and Reproductive Health Issues and Associated Factors in Alamata High School, Northern Ethiopia. International Journal of Sciences: Basic and Applied Research (IJSBAR). 7(1): 83-92.
- Byers ES, Sullivan LF, Mitra K, Sears HA (2020) Parent- Adolescent Sexual Communication in India: Responses of Middle-Class Parents. Journal of Family Issues. 42(4): 1–23.
- Maina BW, Ushie BA, Kabiru CW (2020) Parent-child sexual and reproductive health communication among very young adolescents in Korogocho informal settlement in Nairobi, Kenya. Reprod Health. 17(1): 79.
- Agrawal S, Fatma A, Singh CM. A study of knowledge and attitude of adolescent girls towards reproductive health and related problems. Indian J Prey Soc Med.2007; 38(1, 2): 36-41.
- Ahmed M, Kusuma ML (2016) Knowledge, and attitude of pre- university adolescent girls regarding STDs/ HIV and sexual health in Mysore city. Int J Med Sci Public Health. 5(12): 2452- 56.
- Kusheta S, Bancha B, Habtu Y, Helamo D, Yohannes S (2019) Adolescent-parent communication on sexual and reproductive health issues and its factors among secondary and preparatory school students in Hadiya Zone, Southern Ethiopia: institution based cross sectional study. BMC Pediatr. 19(1): 9.
- Vongsavanh V, Lan VTH, Sychareun V (2020) Sexual and reproductive health communication between parents and high school adolescents in Vientiane Prefecture, Lao PDR. Glob Health Action. 13(sup2): 1785145.
- Soltani F, Sattari M, Parsa P, Farhadian M (2017) Sources of Adolescents' Information about Sexual and Reproductive Health: Gender Similarities and Differences. J. Pharm. Sci. & Res. 9(9): 1624-1628.
- Shiferaw K, Getahun F, Asres G (2014) Assessment of adolescents' communication on sexual and reproductive health matters with parents and associated factors among secondary and preparatory schools' students in Debremarkos town, Northwest Ethiopia. Reprod Health. 11(1): 2.
- Dessie Y, Berhane Y, Worku A (2015) Parent-Adolescent Sexual and Reproductive Health Communication Is Very Limited and Associated with Adolescent Poor Behavioural Beliefs and Subjective Norms: Evidence from a Community Based Cross- Sectional Study in Eastern Ethiopia. PLoS ONE. 10(7): e0129941.
- Moni SA, Nair MK, Devi RS (2013) Pregnancy among unmarried adolescents and young adults. J Obstet Gynaecol India. 63(1): 49- 54.
- Fanta M, Lemma S, Sagaro GG, Meskele M (2016) Factors associated with adolescent–parent communication of reproductive health issues among high school and preparatory students in Boditi town, Southern Ethiopia: a cross-sectional study. Patient Intelligence. 8: 57-70.
- Motsomi K, Makanjee C, Basera T, Nyasulu P (2016) Factors affecting effective communication about sexual and reproductive health issues between parents and adolescents in zandspruit informal settlement, Johannesburg, South Africa. The Pan African Medical Journal. 25: 120.