


Meghadipa Mandal1, Riju Bhattacharyya1, Abhik Banerjee2*
1Consultant Pathologist, Apollo Diagnostics, Regional reference laboratory, Kolkata
2Lab Director and Zonal Technical Chief- East Zone, Apollo Diagnostics, Regional reference laboratory, Kolkata
*Corresponding Author: Abhik Banerjee, Lab Director and Zonal Technical Chief- East Zone, Apollo Diagnostics, Regional reference laboratory, Kolkata.
Introduction
Masson’s tumor or Masson’s hemangioma is also called intravascular papillary endothelial hyperplasia (IPEH). This is a relatively uncommon benign vascular lesion of the skin and subcutaneous tissue. The lesion is frequently confused with angiosarcoma or Kaposis’s sarcoma. Though this entity is not so common, accurate diagnosis is crucial since its clinical appearance may mimic malignant tumors. [1] The disease accounts for approximately 2% of skin and soft tissue vascular tumours. [2]
Case history
A 34-year-old female visited the surgery outpatient department of a charitable hospital in Itanagar, Arunachal Pradesh (Northeast India), complaining of a round to ovoid mass on the palmar side of her left index finger. The lesion was painless and very slowly growing for the last 2 months. On examination, there was a 1.5*1.0 cm firm, round, and nontender lesion on the palmar side of the left hand over the first metacarpophalangeal joint. There was no appreciable change in skin colour, and the lesion was partially mobile. There was no similar lesion anywhere, nor was there any history of similar lesions. There was no history of any fever or other major systemic illness in the last 3 months. The patient was advised of hospitalization and was scheduled for excision of the mass under local anesthesia. The excised lesion was sent to Apollo Diagnostics, regional reference laboratory in Kolkata, for histopathological examination.
A gross examination showed a skin-covered greyish tissue measuring 1.5 * 1*0 cm. All tissue was embedded in one paraffin block and processed per standard operative procedure.
On microscopic examination, sections showed fibro collagenous tissue covered on the surface by the epidermis. The dermis showed a lesion with intravascular papillary proliferation lined by benign, plump endothelial cells. No evidence of mitosis or necrosis was seen. We reported the case as Masson’s Hemangioma (Intravascular Papillary Endothelial Hyperplasia).
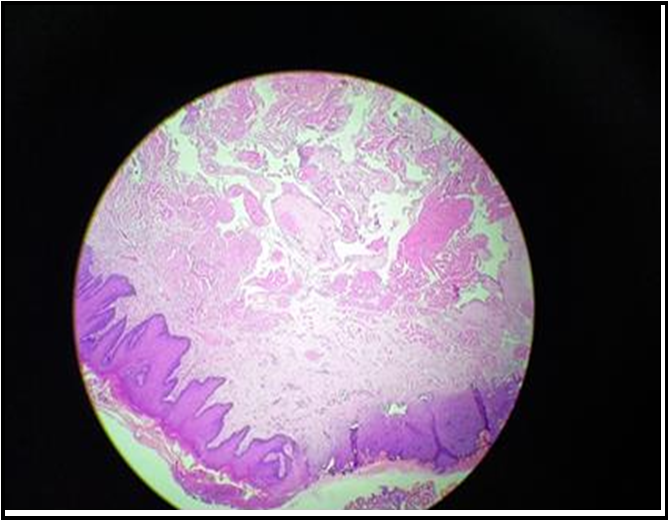
Figure 1. Microscopy showed a skin covered lesion with thick-walled, dilated blood vessels filled with papillary structures projecting into the lumen (H&E 50X)
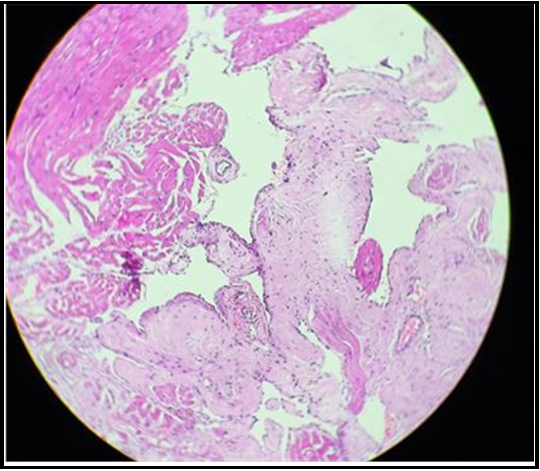
Figure 2. Microscopic section showed a low-power view of papillary proliferation of endothelial cells without any atypia, hyperchromasia, mitosis or necrosis (H & E 100X)
Discussion
IPEH may be found in any part of the body, but the most common locations are hands, fingers, head, and neck. [3] The exact pathogenesis is unclear; however, an unusual thrombus organization following trauma is considered the critical factor as per literature. [4,5] The main stay for diagnosis is histopathological evaluation. The most common and essential differential is angiosarcoma. The main distinguishing finding is the intravascular location of IPEH, whereas angiosarcoma is rarely confined to the vascular lumen. Pyogenic granuloma, Kaposi’s sarcomas are other differentials.
Conclusion
It is critical to distinguish IPEH from other benign or malignant lesions of skin and subcutaneous tissue, especially angiosarcoma, to avoid unnecessary radiation and aggressive resection.
Conflicts of Interest
All the authors declare that they have no competing interests.
References
- Han JW, Lee JH, Kim EK (2019) Intravascular papillary endothelial hyperplasia (Masson's hemangioma) of the face. Arch Craniofac Surg. 20(2): 109-111.
- Guledgud MV, Patil K, Saikrishna D, Madhavan A, Yelamali T (2014) Intravascular papillary endothelial hyperplasia: diagnostic sequence and literature review of an orofacial lesion. Case Rep Dent. 2014:934593.
- Espinosa E, González J, García-Navas F (2017) Intravascular papillary endothelial hyperplasia at foot level: a case report and literature review. The Journal of Foot and Ankle Surgery. 56(1): 72–74.
- Wang CY, Hong CC, Huang ZY, Wang CH (2019) Intravascular papillary endothelial hyperplasia along the intrinsic muscle after hand contusion injury: report of two cases. Acta Orthop Traumatol Turc. 53(2): 154–156.
- Mardani P, Askari A, Shahriarirad R, Ranjbar K, Erfani A, et al. (2020) Masson’s Tumor of the Hand: An Uncommon Histopathological Entity. Case Reports in Pathology. 2020: 4348629.