


Yasser Mohammed Hassanain Elsayed*
Critical Care Unit, Fraskour Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt
*Corresponding author: Elsayed YMH, Critical Care Unit, Fraskour Central Hospital, Damietta Health Affairs, Egyptian Ministry of Health (MOH), Damietta, Egypt
Abstract
Rationale: Coronary artery spasm is a common ischemic heart disease. It is a serious clinical cardiovascular issue. Nitrates such as nitroglycerine have a pivotal role in the management of coronary artery disease.
Patient concerns: A 45-year-old married, officer, heavy smoker, Egyptian male patient presented with acute excruciating severe chest pain and combined electrocardiographic ST-segment coronary artery spasms.
Diagnosis: Combined ST-segment coronary artery spasms of ST-segment elevations and ST-depressions was the most probable diagnosis.
Interventions: Electrocardiogram, echocardiography, and nitroglycerine intravenous infusion.
Outcomes: Dramatic response of both clinical and electrocardiographic combined ST-segment coronary artery spasms to nitroglycerine.
Lessons: A combined ST-segment coronary artery spasms including ST-segment elevation and ST-depression may be present the same ECG. The dramatic efficacy on later using nitroglycerine in the management of combined ST-segment coronary artery spasms.
Keywords: nitroglycerine; coronary artery spasm; combined ST - segment coronary artery spasms; ischemic heart disease
Abbreviations: CAS: Coronary Artery Spasm, ECG: Electrocardiogram, ICU: Intensive Care Unit, NSR: Normal Sinus Rhythm, O2: Oxygen, STEMI: ST-Segment Elevation Myocardial Infarction.
1. Introduction
Coronary Arteries Spasm (CAS) is a cardiovascular entity characterized by chest pain at rest with temporary electrocardiographic (ECG) ischemic ST-segment changes with a prompt response to nitrates. These symptoms are attributed to coronary arteries spasm [1]. This form of angina was first described in 1959 by Prinzmetal et al. [2]. The term of CAS refers to sudden, intense vasoconstriction of an epicardial coronary artery that causes vessel occlusion or near occlusion [3]. The pathophysiology of coronary arteries spasm results from the interaction of 2 components: (1) It is a usually localized, but sometimes diffuse, abnormality of a coronary artery that makes it hyperreactive to vasoconstrictor stimuli, and (2) There is a vasoconstrictor stimulus able to induce the spasm at the level of the hyperreactive coronary segment [3]. The suggested mechanisms of CAS include 1. Presence of endothelial dysfunction, 2. Existence of a primary hyperreactivity of vascular smooth muscle cells (VSMCs), and 3. Other factors may be present [3]. The most common risk factors associated with CAS is smoking. Indeed, active smokers represent about 75% of patients with cases of angina [4]. Why smoking favors CAS, however, remains unknown [3]. Pain decreases with the use of short-acting nitrates. Typically, the chest pain is not triggered by exertion or alleviated with rest as is typical angina [1]. Typically, these patients have ischemic ST-segment changes on an electrocardiogram during an episode of chest discomfort, which returns to baseline on symptom resolution. Transient ST-segment elevation on electrocardiography (ECG) is a characteristic finding in patients with variant angina, However, in more severe cases, ST elevation may be followed by T-wave inversions for hours to days. Most CAS is accompanying with ST-segment depression rather than ST-segment elevation on ECG. CAS plays a pivotal role in the pathogenesis of ischemic heart disease, including stable angina, unstable angina, myocardial infarction, and sudden cardiac death. Arrhythmia, myocardial infarction, and sudden death are the most frequent complications. Coronary angiography may reveal focal spasm of a coronary artery; when coupled with typical symptoms, ECG changes, and even ventricular dysfunction, this spasm may be pathognomonic for the condition. It may also occur in angiographically normal coronary arteries as the so-called 'variant of the variant. Nitrates and calcium channel blockers are the mainstays of medical therapy for vasospastic angina. Calcium antagonist is a first-line treatment due to a vasodilation effect in the coronary vasculature. The use of long- acting nitrates is also effective in preventing vasospastic events. CAS is yielding a dramatic response to the vasodilator action of nitrates. Episodes are usually shortly and quickly alleviated by the administration of nitrates. The ECG abnormalities are temporary and reversible with nitrates. However, nitrates causing vasodilation with dominant venous effects on large capacitance vessels. They also increase coronary collateral circulation, increase aortic compliance, and blood flow to ischemic areas of the myocardium. In addition, nitrates mitigate anginal symptoms by direct impact on the coronary arteries, coronary collateral circulation, aortic compliance and conductance, and blood flow to ischemic areas of the myocardium.
2. Case Presentations
A 45-year-old married, painter, heavy smoker, Egyptian male patient presented with acute severe chest pain. The anxiety was the only associated symptom. Chest pain was anginal, unbearable, and at rest. The patient is a smoker for about 60 cigarettes per day for nearly 17 years. He denied the history of cardiovascular diseases, the same attack, drugs, or any other special habits. Upon general physical examination; generally, the patient was an anxious, severe sweaty, had cold extremities, with a regular heart rate of 78 bpm, blood pressure of 140/100 mmHg, respiratory rate of 20 bpm, the temperature of 36.4 °C, and pulse oximeter of O2 saturation of 98 %. No more relevant clinical data were noted during the clinical examination. He was admitted to the ICU as anginal chest pain and hypertension. Urgent ECG was done that showing mild high lateral ST-segment elevation in (I and aVL) leads and inferior ST-depression depressions in (III and aVF) leads, with normal sinus rhythm (NSR). Serial ECG tracings in ICU showing high lateral ST-segment elevation in (I and aVL) leads and inferior ST-depressions in (III and aVF) leads, and septal ST-depression depressions in (III and aVF) leads with NSR of VR; 78. Gradual resolution of the above ST-elevations and ST- depressions with a gradual decrease in the number of affected leads. O2 inhalation was given (100 %, by nasal cannula, 5 L/min). Pethidine HCL 100 mg given on intermittent IV doses. Aspirin 4 chewable oral tablet (75 mg), clopidogrel 4 oral tablet (75 mg), bisoprolol 1 oral tablet (5 mg), enoxaparin SC injection (60 mg twice daily) was added. Unfortunately, still there was no clinical or electrocardiographic improvement. Intravenous nitroglycerin infusion (7.5 µg/min with intermittent titration) was added. Blood pressure became normalized (130/70 mmHg). Clinical improvement and gradual electrocardiographic of both ST-segment elevations and ST-depressions resolution had happened. The chest pain starts to resolute within 15 minutes after ending streptokinase infusion. The measured random blood sugar was 171 mg/dl. The serial troponin test was negative (less than 0.001 ng/L). Later echocardiography was mild diastolic dysfunction with EF 65% (Figure 4). No more workup was done. Combined ST-segment coronary artery spasms of ST-segment elevation and ST-depression was the most probable diagnosis. The patient was continued on diltiazem tablet (60 mg twice daily), and nitroglycerin retard capsule (2.5 mg twice daily) until discharged on the 2nd day. He continued on diltiazem tablet (60 mg twice daily), and nitroglycerin retard capsule (2.5 mg twice daily). Planning for catheter revascularization was a future option.
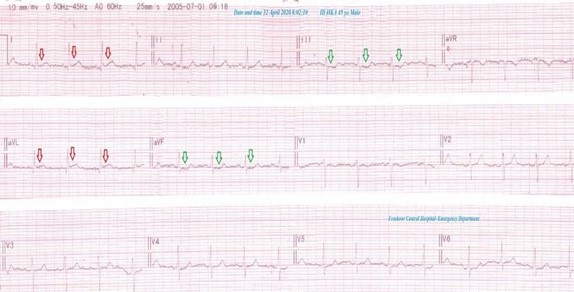
Figure 1: An initial Emergency ECG tracing showing mild high lateral ST-segment elevation in (I and aVL) leads (red arrows) and inferior ST-depression depressions in (III and aVF) leads (green arrows), with normal sinus rhythm of VR;82.
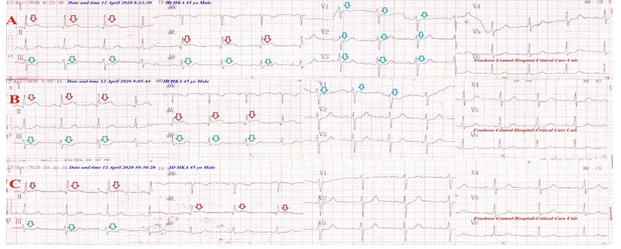
Figure 2: Serial ECG tracings in ICU A. tracing showing high lateral ST-segment elevation in (I and aVL) leads (red arrows) and inferior ST-depressions in (III and aVF) leads (green arrows), and septal ST-depression depressions in (III and aVF) leads (blue arrows) with normal sinus rhythm of VR;78. B and C tracings showing gradual resolution of the above ST-elevations and ST-depressions with a gradual decrease in the number of affected leads.
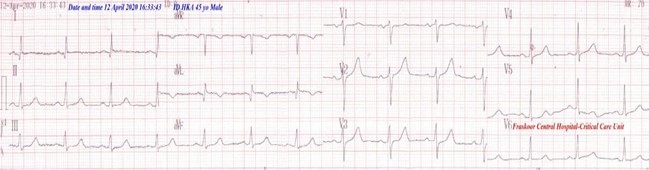
Figure 3: ECG tracing showing complete electrocardiographic ST-segment normalization of the above elevations and ST-depressions with normal sinus rhythm of VR;70.
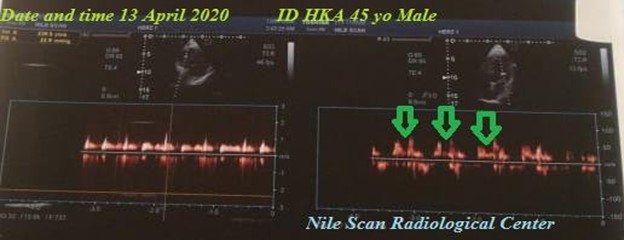
Figure 4: Echocardiography image showing evidence of mild diastolic dysfunction (green arrows).
3. Discussion
-
Overview: A 45-year-old heavy smoker male patient presented with anginal severe chest pain at rest. An electrocardiographic combined ST-segment coronary artery spasms including ST- segment elevation and ST-depression was the hallmark of the current case.
-
I can’t compare the current case with similar conditions. There are no similar or known cases with the same management for near comparison.
-
Study question here; How did combined ST-segment coronary artery spasms with ST-segment elevation and ST-depression in the same ECG?
-
The primary objective for my case study was the presence of anginal severe chest pain at rest and combined ST-segment coronary artery spasms in ECG. Smoking was a major risk factor.
-
The secondary objective for my case study was the initial resistance of the case to standard anginal treatment.
-
The dramatic efficacy on later using nitroglycerine in the management of combined ST-segment coronary artery spasms.
-
The author thinks that the unbearable anginal pain may correlate specifically to lateral coronary artery spasms.
-
The acute high lateral ST-segment elevation myocardial infarction (STEMI) is the main differential diagnosis.
4. Limitations of the Study
-
There are no known limitations in the study.
5. Conclusion and Recommendations
-
A combined ST-segment coronary artery spasms including ST-segment elevation and ST-depression may be present the same ECG.
-
Also, it is recommended to extend the research on the impact of nitroglycerine in the management of both clinical and electrocardiographic combined ST-segment coronary artery spasms.
6. Acknowledgment
-
The author wishes to thank the critical care unit nurses who make extra ECG copies for helping me.
7. Conflicts of Interest
-
There are no conflicts of interest.
References
-
Ziccardi MR, Hatcher JD (2019) Prinzmetal Angina. StatPearls [Internet].
-
Lanza GA, Careri G, and Crea F (2011) Mechanisms of Coronary Artery Spasm. Circulat 124: 1774-1782.
-
Sugiishi M, Takatsu F (1993) Cigarette smoking is a major risk factor for CAS. Circulat 87: 76-79.
-
Liu PC, Cheng CW, Hung MJ; Chen SJ, Yang NI, et al. (2010) Variant Angina with Angiographically Normal or Near- normal Coronary Arteries: A 10-year Experience. J lntern Med Taiwan. 21: 79-89.