


Emilia Albinița Cuc¹, Gabriela Ciavoi¹, Diana Berechet¹*, Mihai Benchea¹, George Daniel Cuc²
¹Department of Dental Medicine, Faculty of Medicine and Pharmacy, University of Oradea, Romania
²Faculty of Medicine, University of Medicine and Pharmacy “Iuliu Hatieganu”, Cluj Napoca, România, 400347
*Corresponding Author: Diana Berechet, Assistant Professor, MD, PhD, Department of Dental Medicine, Faculty of Medicine and Pharmacy, University of Oradea, Universităţii Street, 410087 Oradea, Romania
Abstract
Reduced hypodontia may be considered an expression of phylogenetic reduction or associated with other abnormalities. Reduced hypodontia is related to permanent dentition, and the characteristic disorders occur at the arcade and can lead to vocal impairment and facial expression and functions. It is often encountered in the mandibular lateral incisor, mandibular second premolar, and third molar end-of-series terminals, but it can also occur in the canine. The canine agenesis is very rare, ranging from 0.07 to 0.13%.
This study presents the case of a 17-year-old female patient with bilateral maxillary canine agenesis, upper lateral incisor aplasia, and second lower molar aplasia, lower canines included. Following the clinical and radiographic examination, treatment options were discussed.
Keywords: agenesis, hypodontia, canine
Introduction
Dental agenesia or anodontia is the congenital absence of the dental bud and, subsequently, the missing of the corresponding tooth on the arch, being one of the dental anomalies of number. It is often associated with other oro-dental anomalies such as cleft lip and palate, enamel hypoplasia, etc. The incidence of this anomaly is influenced by the type of dentition (i.e., temporary/permanent), gender, demographic, and geographic factors, but it has been found that there is also a genetic, hereditary component involved. Hypodontia - numerical teeth reduction may affect isolated teeth or entail a complete absence of dental buds (anodontia). It has been suggested that hypodontia is not only the most common dental anomaly but it also generates a large number of clinical complications that are not very easy to treat.[1]
The frequency of this abnormality is estimated to be around 4-5%. Hypodontia cases are considered phylogenetic by reducing the end-of-series teeth (wisdom teeth, second premolars, lateral incisors). This tendency to reduce the number and size of the teeth causes the disappearance of the wisdom teeth in 25% of all cases, followed by the lateral incisors in 12% and the premolars in 11% of the groups of patients with hypodontia. Permanent dentition is more frequently affected than the temporary one [2,3]. Epidemiological data show that the anomaly is present in the population in a share of 1.5-3%, and it has a frequency of 4.3% among other dental-maxillary abnormalities [4].
The prevalence of congenitally missing teeth (from now on CMT) in the general population was reported as ranging between 0.027% and 10.1%, with significant variations depending on geographical areas and race [5,6]. In the general population, the lower second premolar is the most common missing tooth, followed by the lateral incisor and the mandibular second premolar [7]. A higher frequency was observed in the case of girls than in boys [7,8].
Hypodontia is frequently associated with maxillary dental developmental abnormalities (MDDA) and positional disorders of the teeth in place. [3-5] Agenesis of permanent canines in a non-syndromic patient is extremely rare. [6-8]
Case Presentation
The case presented herein describes a rare form of hypodontia, namely the bilateral agenesis of the maxillary, the upper lateral incisors associated with that permanent canines agenesis, and the agenesis of the lower second permanent molars. The absence of the buds of the third molars, both upper and lower, is also noted.
The 17-year-old female patient presented to the dental office for physiological reasons. The patient’s personal medical history is irrelevant. At clinical examination, we noticed the patient’s oval face, attenuated nasolabial folds, enhanced mental foramen, smaller lower facial height, positive ratio of the lips in positive lip step, convex facial profile with decreased lower facial height (see Figure no.1).
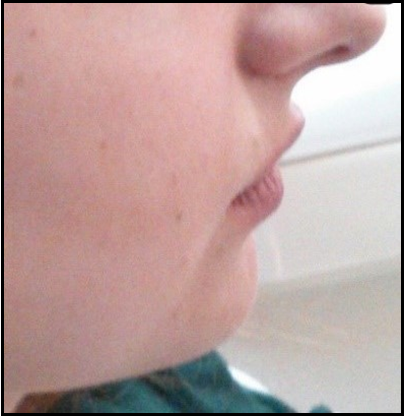
Figure 1: Lateral examination
Buccal mucosa examination showed a normal appearance and colouring. The patient presents a class II anomaly and canine and molar distalizations were reported (see Figure no.2,3,4).

Figure.2 Dental arch aspect

Figure.3 Right hemiarch: presence of 5.2 and 5.3

Figure.4 Second hemiarc: presence of 6.2 and 6.3
The presence of temporary teeth is noted in the teeth inventory: bilateral lateral incisors 5.2, 6.2, presence of upper temporary canines 5.3, 6.3, and presence of temporary canines 7.3, 8.3 in lower arch (see Figure no.5,6).

Figure.5 Upper arch

Figure.6 Lower arch aspect
Considering the age of the patient and the dental eruption timetable, during the clinical examination we presumed the absence of permanent teeth from the arch, and we recommended the patient to undergo OPG and CBCT. Patient’s oral hygiene was satisfactory, and the clinical examination showed the absence of carious lesions. The radiological examination on the orthopantomogram (OPG) shows the absence of dental buds of upper lateral incisors and canines on both dental hemiarchs (1.2 and1.3, and 2.2 and 2.3), as well as the absence of the lower second molar buds are absent (3.7 and 4.7), and teeth 3.3 and 4.3 in lower arch are included (see Figure no.7).
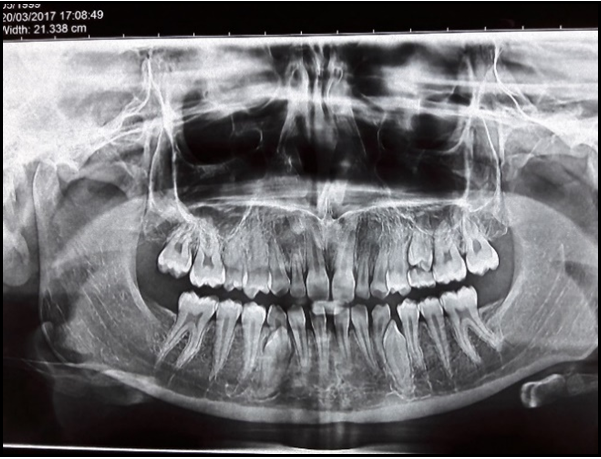
Figure 7: Ortopantomograma examination
Both the temporary lateral incisors and the temporary canines did not show any degree of root regrowth/risalisa.
Radiological CBCT also highlights the lack of permanent teeth buds, as well as the presence of canines included in the lower arcade (see Figure no.8,9).
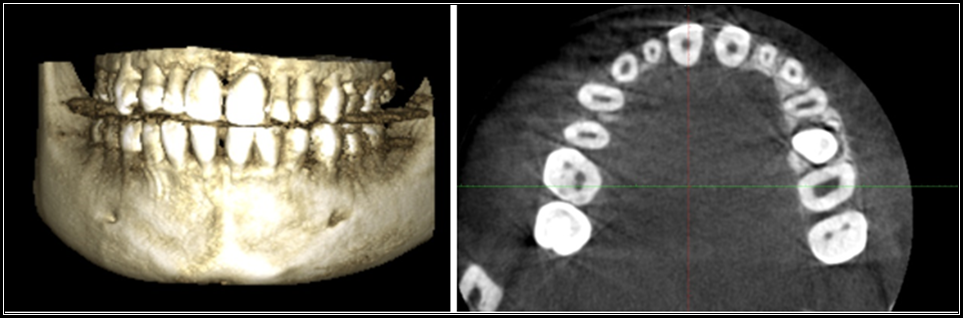
Figure.8 CBCT examination of the upper arch
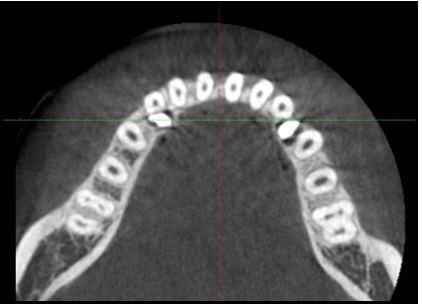
Figure 9: CBCT examination of the lower arch
The patient was monitored for approx. one year, but there were no significant resorption changes at the level of the roots of the temporary teeth - upper lateral incisors and upper canines, and a slight root resorption occurred only in the lower arch at the level of 73 and 83, i.e., in the temporary canines. It is worth mentioning that the subject’s sister did not show any form of hypodontia.
he dental treatment plan conceived consisted of extracting the temporary lateral incisors and replacing them with two implant-prosthetic restorations after the completion of the facial growth. Considering the lifespan of the quick canines, the patient’s age, and growth potential, it was decided to maintain teeth and replace them with implants only later. [9]. Another option considered is the replacement of temporary canines with upper first premolars to reduce the edentulous space. [10] It is recommendable to avoid inserting implants in the maxillary canine area due to the functional trauma in this area [10,11], but there were cases in which temporary canines were replaced with implants. [12]
As for the mandibular arch, it was decided to extract the temporary canines and direct the eruption of the permanent canines. The use of mini-implants would help close the spaces by mesialization of the lateral teeth.
Discussion
In temporary dentition, hypodontia is very rare, ranging between 0.1% and 2.4% [13,14,15], with females being more affected than males, i.e., a male: female ratio of 2:3. As regards the unilateral or bilateral missing of teeth, Endo et al. [11] reported that 89% of patients had bilateral missing teeth. The lateral incisor hypodontia can be accompanied by diastema. In mixed dentition, the anomaly is suspected whenever the temporal lateral incisor persists, or eruption disorders occur with the premolar eruption before the lateral incisor, and the presence of a false diastema [12] Canine agenesia has been reported in sporadic cases, for example in a study conducted in India by Guttal et al. in 2010, Gupta et al. in 2011 and Shetty et al in 2012, no cases of agenesis of canine were reported. It may also be associated with other dental anomalies such as microdontia, supernumerary teeth, or other teeth missing malocclusions [13,14]. In other studies, the prevalence of canine agenesis ranges between 0.07 and 0.13% (Kambalimath et al., 2015) [15].
Treatment can sometimes be challenging to apply and requires interdisciplinary collaboration between the pediatric dentist, orthodontist, surgeon, and prosthetician. A key-role lies with the pediatric dentist, who has to evaluate the number of missing teeth and the number of temporary teeth remaining on the arch to plan the treatment. The presence of an associated abnormality, the degree of ingress, and the facial profile of the patient are other factors in making a therapeutic decision. If the roots of the teeth face root resorption problems, they can be extracted, and one may maintain the space by a space maintainer that will restore physiological and phonetic function until around the age of 20, when bridges or dental implants can be applied. In this situation, the option was to keep the temporary teeth in the arch and perform periodic dental checks to track root resorption. It is recommended to devitalize temporary teeth to maintain them longer on the hook. If root resorption occurs, it is possible to opt for extraction followed by implant prosthetic treatment.
Frequently, due to their location at the front of the arches, dental anomalies can create serious aesthetic and physiognomic problems in patients. Prosthetic treatment is the best solution from a physiognomic and durability point of view, but it can only be carried out after a certain age, given the loss of dental tissue for tooth preparation [14]. In children and adolescents, until the end of the growth period, which is considered at the age of 18 years, conservative, less invasive methods should be considered, often for a shorter period or even permanent [14].
Regarding frequency, studies have shown that the upper lateral incisor is the second missing tooth after the lower second premolar in the total number of missing teeth [15]. The absence of these teeth may be influenced by ethnicity, the age of the study group in the case of those with two missing teeth, and the size of the study sample [16].
Females were found to have a higher prevalence than males. The most commonly affected teeth were mandibular second premolars, maxillary lateral incisors, and maxillary second premolars. [17,18]
Regarding prevalence by sex, the prevalence was higher in women than in men (combined OR 1.22; 95% CI: 1.14, 1.30). Regarding teeth, the lower second premolar was the most common missing tooth, followed by the upper lateral incisor and upper second premolar. [18,19]
Conclusions
Dental agenesia or anodontia is the congenital absence of the dental bud and, subsequently, the missing of the corresponding tooth on the arch, being one of the dental anomalies of number. To confirm diagnosis, the most crucial diagnosis used is CBCT, followed by the clinical examination. These cases require close collaboration between a pediatric dentist and a dental surgeon to find the best solution available in terms of treatment.
For the best possible treatment encompassing long-term results, there should be considered the underlying conditions of the patient, if applicable, the type of associated anomaly, the life span of the temporary teeth, the prosthetic reconstruction according to the patient’s preferences, as well as treatment costs.
Conflict of Interests: The authors hereby represent that they have no conflict of interests to declare.
This authors contributed equally to this manuscript/work.
References
- Amini F, Rakhshan V, Babaei P (2012) Prevalence and pattern of hypodontia in permanent dentition of 3374 Iranian orthodontic patients. Dent Res J (Isfahan). 9(3): 245–250.
- Cuc EA. Incidence of dento-maxillary anomalies during mixed dentition period, PhD Thesis, University of Oradea, Romania, 2014
- Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N (2010) Non-syndromic hypodontia in an Iranian orthodontic population. J Oral Sci. 52(3): 455–61.
- Matalova E, Fleischmannova J, Sharpe PT, Tucker AS (2008) Tooth agenesis: from molecular genetics to molecular dentistry. J Dent Res. 87(7): 617–23.
- Cobourne MT (2007) Familial human hypodontia--is it all in the genes? Br Dent J. 203(4): 203-8.
- Bergendal B, Bergendal T, Hallonsten AL, Koch G, Kurol J, et al. (1996) A multidisciplinary approach to oral rehabilitation with osseointegrated implants in children and adolescents with multiple aplasia. Eur J Orthod. 18(2): 119–29.
- Mattheeuws N, Dermaut L, Martens G (2004) Has Hypodontia Increasedin Caucasians During The 20th Century?A Metaanalysis. Eur J Orthod. 26(1): 99-103.
- Brook Ah (1975) Variables And Criteria In Prevalence Studies of Dental Anomaliesof Number, Form and Size. Community Dent Oral Epidemiol. 3(6): 288-293.
- Haselden K, Hobkirk JA, Goodman JR, Jones SP, Hemmings KW (2001) Root resorption in retained deciduous canine and molar teeth without permanent successors in patients with severe hypodontia. Int J Paediatr Dent. 11(3): 171–8.
- Borzabadi-Farahani A (2012) Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J Implantol oral. 38(6): 779– 91.
- Borzabadi-Farahani A, Zadeh HH (2015) Adjunctive orthodontic applications in dental implantology. J Oral Implantol. 41(4): 501-8.
- Mazor Z, Peleg M, Redlich M (1999) Immediate placement of implants in extraction sites of maxillary impacted canine teeth. J Am Dent Asoc. 130(12): 1767–70.
- Guttal K, Naikmasur V, Bhargava P, Bathi RJ (2010) Frequency of developmental dental anomalies in the indian population. Eur J Dent. 4(3): 263–269.
- Kinzer G, Kokich V (2005) Gestionarea incisivilor laterali lipsă în mod congenital. Partea a II-a: Restaurări susținute de dinți. J. De Stomatol. Estet. Și Restaur. 17: 76–84.
- Fukuta Y, Totsuka M, Takeda Y, Yamamoto H (2004) Congenital absence of the permanent canines: a clinico- statistical study. J Oral Sci. 46(4): 247–52.
- Chafaie A (2016) Esthetic management of anterior dental anomalies: A clinical case. International Orthodontics. 14(3): 357-365.
- Rakhshan V (2015) Meta-Analysis of Observational Studies on the Most Commonly Missing Permanent Dentition (Excluding the Third Molars) in Non-Syndromic Dental Patients or Randomly-Selected Subjects, and the Factors Affecting the Observed Rates. J Clin Pediatr Dent. 39(3): 199-207.
- Khalaf K, Miskelly J, Voge E, Macfarlane TV (2014) Prevalence of hypodontia and associated factors: a systematic review and metaanalysis. J Orthod. 41(4): 299-316.
- Nordgarden H, Jensen JL, Storhaug K (2002) Reported prevalence of congenitally missing teeth in two Norwegian counties, Community Dent Health. 19(4): 258-61.